Vaccine Education
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

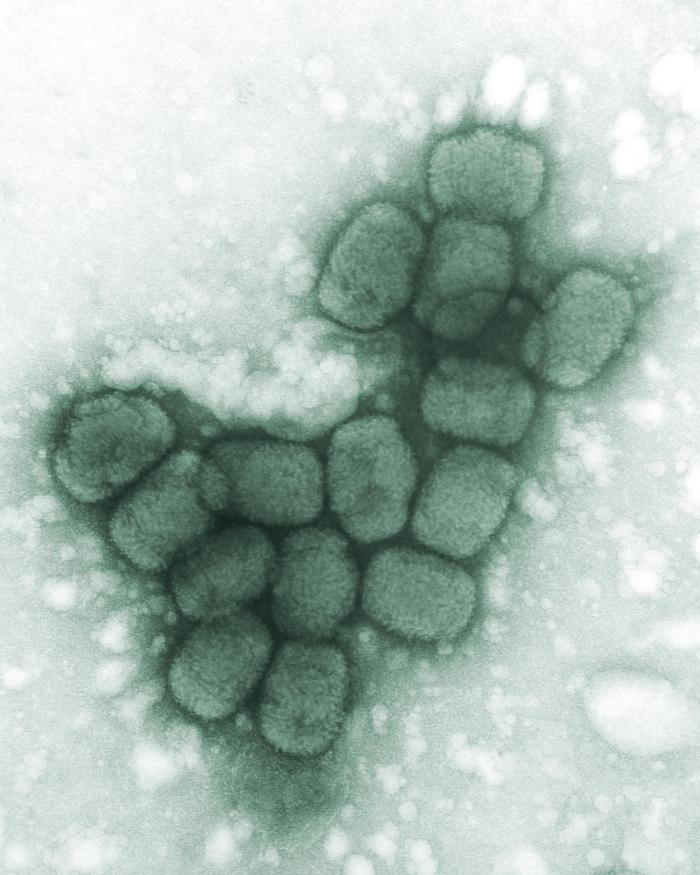
Dr. Schreiber of San Augustine giving a typhoid inoculation at a rural school, San Augustine County, Texas, in April 1943. This image is a work of an employee of the United States Farm Security Administration or Office of War Information domestic photographic units, taken as part of that person's official duties. As a work of the U.S. federal government, the image is in the public domain in the United States. Background image: This is a transmission electron microscopic (TEM) image of a cluster of smallpox viruses, which had been processed using a negative stain technique. See PHIL 2294 for a black and white version of this digitally-colorized image.
Dr. Schreiber of San Augustine giving a typhoid inoculation at a rural school, San Augustine County, Texas, in April 1943. This image is a work of an employee of the United States Farm Security Administration or Office of War Information domestic photographic units, taken as part of that person's official duties. As a work of the U.S. federal government, the image is in the public domain in the United States. Background image: This is a transmission electron microscopic (TEM) image of a cluster of smallpox viruses, which had been processed using a negative stain technique. See PHIL 2294 for a black and white version of this digitally-colorized image.
Dr. Schreiber of San Augustine giving a typhoid inoculation at a rural school, San Augustine County, Texas, in April 1943. This image is a work of an employee of the United States Farm Security Administration or Office of War Information domestic photographic units, taken as part of that person's official duties. As a work of the U.S. federal government, the image is in the public domain in the United States. Background image: This is a transmission electron microscopic (TEM) image of a cluster of smallpox viruses, which had been processed using a negative stain technique. See PHIL 2294 for a black and white version of this digitally-colorized image.
How, why, when, and for what we vaccinate today starts with the story of smallpox, polio, and diphtheria. Our whole understanding of how vaccine immunity works began with the discovery of the relationship between smallpox and cowpox. This one thing alone resulted in an inestimable number of lives saved in the last two hundred years.
This course is designed to give accurate information for parents. We recognize (and support) the right to refuse vaccines contrary to medical advice. But we also know that many times, parents seem to opt out because they don't know the facts about what vaccines do, what they actually contain, and why we think they are so important.
It is best viewed on a desktop computer, and I strongly encourage you to take notes. I do not suggest that children view the content!
After you view all the slides, you'll end up back here where you can click on the button to take the open book quiz. There are 20 questions pulled randomly from a pool of almost 100. Some questions are worth more points. You can view the slides anytime and take the quiz as many times as you need to.
Any video material will NOT be on the quiz. Click the right slide arrow to begin. The last slide has the link to the quiz.
How, why, when, and for what we vaccinate today starts with the story of smallpox, polio, and diphtheria. Our whole understanding of how vaccine immunity works began with the discovery of the relationship between smallpox and cowpox. This one thing alone resulted in an inestimable number of lives saved in the last two hundred years.
This course is designed to give accurate information for parents. We recognize (and support) the right to refuse vaccines contrary to medical advice. But we also know that many times, parents seem to opt out because they don't know the facts about what vaccines do, what they actually contain, and why we think they are so important.
It is best viewed on a desktop computer, and I strongly encourage you to take notes. I do not suggest that children view the content!
After you view all the slides, you'll end up back here where you can click on the button to take the open book quiz. There are 20 questions pulled randomly from a pool of almost 100. Some questions are worth more points. You can view the slides anytime and take the quiz as many times as you need to.
Any video material will NOT be on the quiz. Click the right slide arrow to begin. The last slide has the link to the quiz.
How, why, when, and for what we vaccinate today starts with the story of smallpox, polio, and diphtheria. Our whole understanding of how vaccine immunity works began with the discovery of the relationship between smallpox and cowpox. This one thing alone resulted in an inestimable number of lives saved in the last two hundred years.
This course is designed to give accurate information for parents. We recognize (and support) the right to refuse vaccines contrary to medical advice. But we also know that many times, parents seem to opt out because they don't know the facts about what vaccines do, what they actually contain, and why we think they are so important.
It is best viewed on a desktop computer, and I strongly encourage you to take notes. I do not suggest that children view the content!
After you view all the slides, you'll end up back here where you can click on the button to take the open book quiz. There are 20 questions pulled randomly from a pool of almost 100. Some questions are worth more points. You can view the slides anytime, and take the quiz TWICE in case you fail the first time. A passing score is an A or B. You will only get a final score. We expect you to study!
Any video material will NOT be on the quiz. Click the right slide arrow to begin. The last slide has the link to the quiz.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Photographed in the Republic of Benin, formerly known as Dahomey, sometime during the 1970s worldwide Smallpox Eradication Campaign, this image depicted a small child suffering with a case of smallpox, so severe, that the maculopapular pustules had coalesced over the child’s entire body. Public domain.
Photographed in the Republic of Benin, formerly known as Dahomey, sometime during the 1970s worldwide Smallpox Eradication Campaign, this image depicted a small child suffering with a case of smallpox, so severe, that the maculopapular pustules had coalesced over the child’s entire body. Public domain.
Photographed in the Republic of Benin, formerly known as Dahomey, sometime during the 1970s worldwide Smallpox Eradication Campaign, this image depicted a small child suffering with a case of smallpox, so severe, that the maculopapular pustules had coalesced over the child’s entire body. Public domain.
Smallpox is estimated to have killed 300 to 500 million people worldwide over the history of the infection. There are two forms resulting from slightly different strains of the virus, and one is much more serious than the other.
Exposure occurs from direct, prolonged personal contact with body fluids. Even today, the simple lack of understanding of general contagion along with the various day-to-day local geographic practices propel the spread of disease this way. Ebola is a prime example. It took a lot of education to break social mores about handling the bodies of those who died from it.
Similar to measles, smallpox incubation averages 12 to 14 days and ranges from 7 to 17 days. Raised bumps develop and progress to pus-filled blisters that crust and scab, eventually leaving a pitted scar. Like the flu, smallpox begins with high fever, headache and body aches, and sometimes vomiting, making it difficult to distinguish between them and prevent spread early on.
It kills 30% of those it infects and has the highest mortality rate of any virus. It was finally declared eradicated from the wild in 1980.
Smallpox is estimated to have killed 300 to 500 million people worldwide over the history of the infection. There are two forms resulting from slightly different strains of the virus, and one is much more serious than the other.
Exposure occurs from direct, prolonged personal contact with body fluids. Even today, the simple lack of understanding of general contagion along with the various day-to-day local geographic practices propel the spread of disease this way. Ebola is a prime example. It took a lot of education to break social mores about handling the bodies of those who died from it.
Similar to measles, smallpox incubation averages 12 to 14 days and ranges from 7 to 17 days. Raised bumps develop and progress to pus-filled blisters that crust and scab, eventually leaving a pitted scar. Like the flu, smallpox begins with high fever, headache and body aches, and sometimes vomiting, making it difficult to distinguish between them and prevent spread early on.
It kills 30% of those it infects and has the highest mortality rate of any virus. It was finally declared eradicated from the wild in 1980.
Smallpox is estimated to have killed 300 to 500 million people worldwide over the history of the infection. There are two forms resulting from slightly different strains of the virus, and one is much more serious than the other.
Exposure occurs from direct, prolonged personal contact with body fluids. Even today, the simple lack of understanding of general contagion along with the various day-to-day local geographic practices propel the spread of disease this way. Ebola is a prime example. It took a lot of education to break social mores about handling the bodies of those who died from it.
Similar to measles, smallpox incubation averages 12 to 14 days and ranges from 7 to 17 days. Raised bumps develop and progress to pus-filled blisters that crust and scab, eventually leaving a pitted scar. Like the flu, smallpox begins with high fever, headache and body aches, and sometimes vomiting, making it difficult to distinguish between them and prevent spread early on.
It kills 30% of those it infects and has the highest mortality rate of any virus. It was finally declared eradicated from the wild in 1980.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

This 1968 photograph depicted a view of the right eye of a person who’d contracted smallpox, which had manifested in what was a corneal ulcer, as well as the classical maculopapular rash. See PHIL 10463 for a another view of the corneal ulcer. Public domain.
Background: “The recent smallpox epidemic in Montreal – vaccinating American-bound passengers on a train of the Grand Trunk Railway,” James Marvin, 1885. Osler Library Prints Collection.
This 1968 photograph depicted a view of the right eye of a person who’d contracted smallpox, which had manifested in what was a corneal ulcer, as well as the classical maculopapular rash. See PHIL 10463 for a another view of the corneal ulcer. Public domain.
Background: “The recent smallpox epidemic in Montreal – vaccinating American-bound passengers on a train of the Grand Trunk Railway,” James Marvin, 1885. Osler Library Prints Collection.
This 1968 photograph depicted a view of the right eye of a person who’d contracted smallpox, which had manifested in what was a corneal ulcer, as well as the classical maculopapular rash. See PHIL 10463 for a another view of the corneal ulcer. Public domain.
Background: “The recent smallpox epidemic in Montreal – vaccinating American-bound passengers on a train of the Grand Trunk Railway,” James Marvin, 1885. Osler Library Prints Collection.
Among the 70% of infected individuals that survived smallpox, corneal ulcerations was a common occurrence. This resulted in permanent damage and even blindness.
Smallpox was a serious scourge then. Because we don’t see it in the wild today, the significance of vaccines is more easily discounted.
Outbreaks occurred everywhere, and many efforts to fight smallpox were local. The background image shows vaccination on a train in Montreal, Canada bound for the US.
Were smallpox to reemerge in the world, the landscape of anti-vaccine sentiment would change overnight. It would dwarf the SARS-CoV-2 pandemic.
Among the 70% of infected individuals that survived smallpox, corneal ulcerations was a common occurrence. This resulted in permanent damage and even blindness.
Smallpox was a serious scourge then. Because we don’t see it in the wild today, the significance of vaccines is more easily discounted.
Outbreaks occurred everywhere, and many efforts to fight smallpox were local. The background image shows vaccination on a train in Montreal, Canada bound for the US.
Were smallpox to reemerge in the world, the landscape of anti-vaccine sentiment would change overnight. It would dwarf the SARS-CoV-2 pandemic.
Among the 70% of infected individuals that survived smallpox, corneal ulcerations was a common occurrence. This resulted in permanent damage and even blindness.
Smallpox was a serious scourge then. Because we don’t see it in the wild today, the significance of vaccines is more easily discounted.
Outbreaks occurred everywhere, and many efforts to fight smallpox were local. The background image shows vaccination on a train in Montreal, Canada bound for the US.
Were smallpox to reemerge in the world, the landscape of anti-vaccine sentiment would change overnight. It would dwarf the SARS-CoV-2 pandemic.

- The story of vaccines and vaccination begins with smallpox.
- Smallpox is the deadliest viral scourge in history, with estimates ranging between 300-500 million dead for all time.
- There are two main types of smallpox.
- Transmission occurs through contact with infectious body fluids.
- Symptoms include high fever, headache, body aches, followed by raised, pus-filled, crusty blisters that produce scabs.
- The mortality rate of smallpox is around 30%, while Ebola kills around 70% of infected individuals.
- Corneal ulceration is a common occurrence in survivors and can result in blindness.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

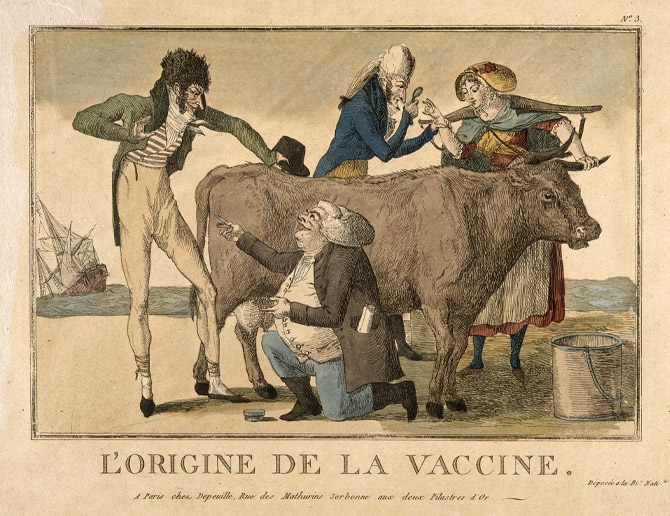
The story of how we defeated the virus started with Edward Jenner and English milkmaids a hundred years earlier. Milkmaids contracted cowpox from milking cows infected with cowpox. Symptoms were similar to smallpox, but it was not fatal. Jenner (and others) noticed that milkmaids who had already been infected with cowpox were immune to smallpox.
Sarah Nelmes was such a milkmaid. On May 14, 1796, Jenner applied material from one of Sarah’s hand lesions to two superficial incisions on 8-year-old James Phipps, a child who had never had smallpox. James developed evidence of infection, which was slight, and quickly recovered.
On July 1, 1796, Jenner then exposed James to smallpox, but he did not develop the disease. He published his account, and that is where cowpox got the official name “variolae vaccinae.” The term “virus” came from Roman times and referred to a noxious agent or poison. No one knew what a virus was at that time, however. Infectious agents were simply known to cause disease by spreading from infected people to uninfected people.
What Jenner had discovered was that cowpox and smallpox were of such close molecular similarity, that infection with the milder cowpox prevented the more serious infection of smallpox. It was Jenner who coined the terms vaccine and vaccinations.
The story of how we defeated the virus started with Edward Jenner and English milkmaids a hundred years earlier. Milkmaids contracted cowpox from milking cows infected with cowpox. Symptoms were similar to smallpox, but it was not fatal. Jenner (and others) noticed that milkmaids who had already been infected with cowpox were immune to smallpox.
Sarah Nelmes was such a milkmaid. On May 14, 1796, Jenner applied material from one of Sarah’s hand lesions to two superficial incisions on 8-year-old James Phipps, a child who had never had smallpox. James developed evidence of infection, which was slight, and quickly recovered.
On July 1, 1796, Jenner then exposed James to smallpox, but he did not develop the disease. He published his account, and that is where cowpox got the official name “variolae vaccinae.” The term “virus” came from Roman times and referred to a noxious agent or poison. No one knew what a virus was at that time, however. Infectious agents were simply known to cause disease by spreading from infected people to uninfected people.
What Jenner had discovered was that cowpox and smallpox were of such close molecular similarity, that infection with the milder cowpox prevented the more serious infection of smallpox. It was Jenner who coined the terms vaccine and vaccinations.
The story of how we defeated the virus started with Edward Jenner and English milkmaids a hundred years earlier. Milkmaids contracted cowpox from milking cows infected with cowpox. Symptoms were similar to smallpox, but it was not fatal. Jenner (and others) noticed that milkmaids who had already been infected with cowpox were immune to smallpox.
Sarah Nelmes was such a milkmaid. On May 14, 1796, Jenner applied material from one of Sarah’s hand lesions to two superficial incisions on 8-year-old James Phipps, a child who had never had smallpox. James developed evidence of infection, which was slight, and quickly recovered.
On July 1, 1796, Jenner then exposed James to smallpox, but he did not develop the disease. He published his account, and that is where cowpox got the official name “variolae vaccinae.” The term “virus” came from Roman times and referred to a noxious agent or poison. No one knew what a virus was at that time, however. Infectious agents were simply known to cause disease by spreading from infected people to uninfected people.
What Jenner had discovered was that cowpox and smallpox were of such close molecular similarity, that infection with the milder cowpox prevented the more serious infection of smallpox. It was Jenner who coined the terms vaccine and vaccinations.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
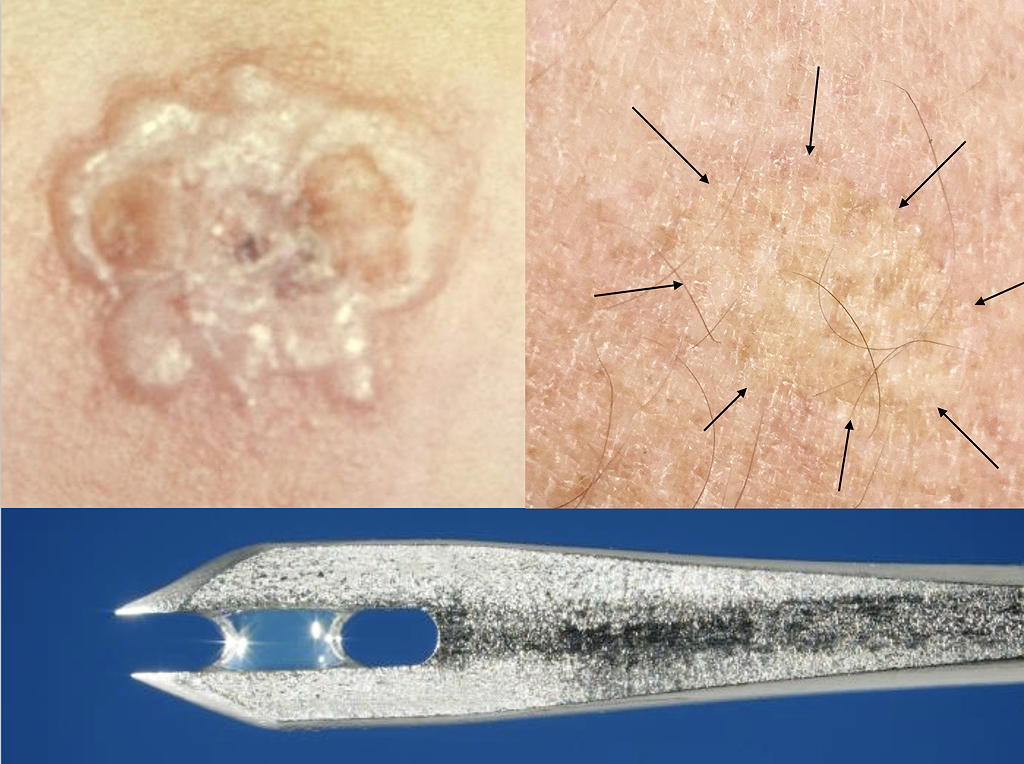
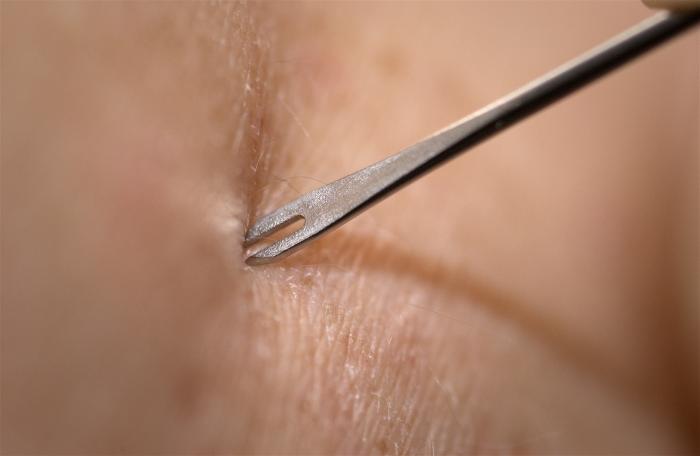
This photograph depicts a magnified view of the tip of a bifurcated needle, used to vaccinate individuals against smallpox. Some vaccine solution can be seen clinging to the tip of the needle, ready to be administered to a vaccine recipient. Vaccinia vaccine does not contain smallpox (variola) virus, but does contain live, Vaccinia viral particles.Public domain. Backgound Photo Credit: James Gathany Content Providers(s): CDC - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #2841. Public domain.
This photograph depicts a magnified view of the tip of a bifurcated needle, used to vaccinate individuals against smallpox. Some vaccine solution can be seen clinging to the tip of the needle, ready to be administered to a vaccine recipient. Vaccinia vaccine does not contain smallpox (variola) virus, but does contain live, Vaccinia viral particles.Public domain. Backgound Photo Credit: James Gathany Content Providers(s): CDC - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #2841. Public domain.
This photograph depicts a magnified view of the tip of a bifurcated needle, used to vaccinate individuals against smallpox. Some vaccine solution can be seen clinging to the tip of the needle, ready to be administered to a vaccine recipient. Vaccinia vaccine does not contain smallpox (variola) virus, but does contain live, Vaccinia viral particles.Public domain. Backgound Photo Credit: James Gathany Content Providers(s): CDC - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #2841. Public domain.
The current smallpox vaccine is not manufactured with the actual smallpox virus. It is made from live Vaccinia virus which is similar to both cowpox and smallpox.
This vaccine was not given subcutaneously or intramuscularly like most vaccines are today. It was first administered with a special double-pointed needle dipped into the vaccine solution. The site of the multiple needle pricks to the skin becomes a weepy blister that scabs over after a week.
The lower image shows the double vaccination needle that was initially used to vaccinate individuals. The upper left image is the typical reaction to that vaccination. The top right image is my own vaccination scar.
We know today that those vaccinated like me probably retain immunity from smallpox for about seven years.
The current smallpox vaccine is not manufactured with the actual smallpox virus. It is made from live Vaccinia virus which is similar to both cowpox and smallpox.
This vaccine was not given subcutaneously or intramuscularly like most vaccines are today. It was first administered with a special double-pointed needle dipped into the vaccine solution. The site of the multiple needle pricks to the skin becomes a weepy blister that scabs over after a week.
The lower image shows the double vaccination needle that was initially used to vaccinate individuals. The upper left image is the typical reaction to that vaccination. The top right image is my own vaccination scar.
We know today that those vaccinated like me probably retain immunity from smallpox for about seven years.
The current smallpox vaccine is not manufactured with the actual smallpox virus. It is made from live Vaccinia virus which is similar to both cowpox and smallpox.
This vaccine was not given subcutaneously or intramuscularly like most vaccines are today. It was first administered with a special double-pointed needle dipped into the vaccine solution. The site of the multiple needle pricks to the skin becomes a weepy blister that scabs over after a week.
The lower image shows the double vaccination needle that was initially used to vaccinate individuals. The upper left image is the typical reaction to that vaccination. The top right image is my own vaccination scar.
We know today that those vaccinated like me probably retain immunity from smallpox for about seven years.
- It was noticed in the 1700s in Great Britain that milkmaids who contracted cowpox seemed to be immune to smallpox.
- Cowpox is a minor pustular illness with an appearance similar to smallpox.
- On May 14, 1796, Jenner applied pustular material from Sarah Nelmes, a milkmaid, into superficial incisions on 8-year-old James Phipps, who had never had smallpox.
- Six weeks later, Jenner exposed Phipps to active smallpox, and Phipps failed to develop smallpox as expected.
- Jenner concluded that infection with cowpox somehow produced immunity to smallpox.
- Modern smallpox vaccine uses vaccinia, a minor poxvirus whose lesions resemble both smallpox and cowpow.
- Vaccination was accomplished using variolation done with multiple pricks of a double-pronged, vaccine-dipped needle.
- Vaccination today gives about seven years of immunity.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

An 1802 cartoon of the early controversy surrounding Edward Jenner's vaccination theory, showing using his cowpox-derived smallpox vaccine causing cattle to emerge from patients. Public domain.
An 1802 cartoon of the early controversy surrounding Edward Jenner's vaccination theory, showing using his cowpox-derived smallpox vaccine causing cattle to emerge from patients. Public domain.
An 1802 cartoon of the early controversy surrounding Edward Jenner's vaccination theory, showing using his cowpox-derived smallpox vaccine causing cattle to emerge from patients. Public domain.
Very few experienced symptoms beyond the funny-looking vaccination scar. The 30% mortality of the disease greatly overshadowed any vaccine. Nevertheless, there was no small amount of controversy even then, as you can see from this old parody of the vaccine.
Edward Jenner had a very personal interest in smallpox, which led him in his effort to vaccinate for it. He was born in 1749, orphaned at age 5. When he was a child, it was first postulated that by intentionally infecting healthy children with smallpox, that it could somehow prevent a full-blown case of the disease. He was variolated, i.e. “vaccinated,” with smallpox while at Wotton-under-Edge between Bristol and Gloucester, England.
He suffered only a mild attack of smallpox, though for six weeks he was bled, purged, and then “haltered up” in the inoculation stables with other smallpox victims.
Jenner first heard cowpox could prevent smallpox around age 13 when he was apprenticed as an apothecary. Local community immunity to smallpox depended on the local presence of cowpox—if there was no cowpox, then infection was more prevalent. Jenner understood the need for a vaccine for that reason. All this propelled him to find a better way to prevent smallpox.
Very few experienced symptoms beyond the funny-looking vaccination scar. The 30% mortality of the disease greatly overshadowed any vaccine. Nevertheless, there was no small amount of controversy even then, as you can see from this old parody of the vaccine.
Edward Jenner had a very personal interest in smallpox, which led him in his effort to vaccinate for it. He was born in 1749, orphaned at age 5. When he was a child, it was first postulated that by intentionally infecting healthy children with smallpox, that it could somehow prevent a full-blown case of the disease. He was variolated, i.e. “vaccinated,” with smallpox while at Wotton-under-Edge between Bristol and Gloucester, England.
He suffered only a mild attack of smallpox, though for six weeks he was bled, purged, and then “haltered up” in the inoculation stables with other smallpox victims.
Jenner first heard cowpox could prevent smallpox around age 13 when he was apprenticed as an apothecary. Local community immunity to smallpox depended on the local presence of cowpox—if there was no cowpox, then infection was more prevalent. Jenner understood the need for a vaccine for that reason. All this propelled him to find a better way to prevent smallpox.
Very few experienced symptoms beyond the funny-looking vaccination scar. The 30% mortality of the disease greatly overshadowed any vaccine. Nevertheless, there was no small amount of controversy even then, as you can see from this old parody of the vaccine.
Edward Jenner had a very personal interest in smallpox, which led him in his effort to vaccinate for it. He was born in 1749, orphaned at age 5. When he was a child, it was first postulated that by intentionally infecting healthy children with smallpox, that it could somehow prevent a full-blown case of the disease. He was variolated, i.e. “vaccinated,” with smallpox while at Wotton-under-Edge between Bristol and Gloucester, England.
He suffered only a mild attack of smallpox, though for six weeks he was bled, purged, and then “haltered up” in the inoculation stables with other smallpox victims.
Jenner first heard cowpox could prevent smallpox around age 13 when he was apprenticed as an apothecary. Local community immunity to smallpox depended on the local presence of cowpox—if there was no cowpox, then infection was more prevalent. Jenner understood the need for a vaccine for that reason. All this propelled him to find a better way to prevent smallpox.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Background image. At the time, this 1966 map revealed the worldwide distribution of smallpox, and the countries in which it was endemic. Public domain.
Background image. At the time, this 1966 map revealed the worldwide distribution of smallpox, and the countries in which it was endemic. Public domain.
Background image. At the time, this 1966 map revealed the worldwide distribution of smallpox, and the countries in which it was endemic. Public domain.
This is chickenpox (varicella) before we had the chickenpox vaccine. In healthy children, the vesicles are very itchy and centrally located on the trunk, scalp, and face. The lesions may number from 250 to 500 blisters. Scarring is not uncommon because of the intense itching. In Jenner’s time, it was often confused for Variola minor, the less virulent form of smallpox. It’s hard to tell the difference clinically from the milder manifestation of smallpox.
Don’t be fooled, though. Chickenpox can be terrible itself. Cerebellar ataxia (being wobbly and even unable to walk) occurs in about 1 in 4,000 children. Varicella encephalitis occurred in 1 in 50,000 to 1 in 33,000 cases. Adults with primary chickenpox are far sicker. Infection in pregnancy may leave the unborn child with permanent scarring, aplasia of extremities, chorioretinitis, micrognathia (small jaw), optic atrophy, cataracts, Horner syndrome (droopy eyelid), blindness, mental retardation, fetal herpes zoster and even death.
Because parents were unaware of the significance of chicken pox, albeit in smaller numbers than smallpox, the chickenpox vaccine was easily discounted at first. They would even have chickenpox parties to get their kids infected and have it done with.
This is chickenpox (varicella) before we had the chickenpox vaccine. In healthy children, the vesicles are very itchy and centrally located on the trunk, scalp, and face. The lesions may number from 250 to 500 blisters. Scarring is not uncommon because of the intense itching. In Jenner’s time, it was often confused for Variola minor, the less virulent form of smallpox. It’s hard to tell the difference clinically from the milder manifestation of smallpox.
Don’t be fooled, though. Chickenpox can be terrible itself. Cerebellar ataxia (being wobbly and even unable to walk) occurs in about 1 in 4,000 children. Varicella encephalitis occurred in 1 in 50,000 to 1 in 33,000 cases. Adults with primary chickenpox are far sicker. Infection in pregnancy may leave the unborn child with permanent scarring, aplasia of extremities, chorioretinitis, micrognathia (small jaw), optic atrophy, cataracts, Horner syndrome (droopy eyelid), blindness, mental retardation, fetal herpes zoster and even death.
Because parents were unaware of the significance of chicken pox, albeit in smaller numbers than smallpox, the chickenpox vaccine was easily discounted at first. They would even have chickenpox parties to get their kids infected and have it done with.
This is chickenpox (varicella) before we had the chickenpox vaccine. In healthy children, the vesicles are very itchy and centrally located on the trunk, scalp, and face. The lesions may number from 250 to 500 blisters. Scarring is not uncommon because of the intense itching. In Jenner’s time, it was often confused for Variola minor, the less virulent form of smallpox. It’s hard to tell the difference clinically from the milder manifestation of smallpox.
Don’t be fooled, though. Chickenpox can be terrible itself. Cerebellar ataxia (being wobbly and even unable to walk) occurs in about 1 in 4,000 children. Varicella encephalitis occurred in 1 in 50,000 to 1 in 33,000 cases. Adults with primary chickenpox are far sicker. Infection in pregnancy may leave the unborn child with permanent scarring, aplasia of extremities, chorioretinitis, micrognathia (small jaw), optic atrophy, cataracts, Horner syndrome (droopy eyelid), blindness, mental retardation, fetal herpes zoster and even death.
Because parents were unaware of the significance of chicken pox, albeit in smaller numbers than smallpox, the chickenpox vaccine was easily discounted at first. They would even have chickenpox parties to get their kids infected and have it done with.
- From the start, vaccination for smallpox had its opponents.
- Jenner was motivated to find a cure for smallpox because he was “vaccinated” with active smallpox as a child, though he contracted the less serious form.
- Chickenpox lesions are similar to both smallpox and cowpox.
- There are very, very few physicians alive today who have seen smallpox, so likely it would be misdiagnosed initially, if it reemerged.
- Today, the public at large would easily mistake a case of smallpox for chickenpox.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

CDC/ World Health Organization Stanley O. Foster M.D., M.P.H. - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #7762. Public domain.
CDC/ World Health Organization Stanley O. Foster M.D., M.P.H. - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #7762. Public domain.
CDC/ World Health Organization Stanley O. Foster M.D., M.P.H. - This media comes from the Centers for Disease Control and Prevention's Public Health Image Library (PHIL), with identification number #7762. Public domain.
In late 1975, Rahima Banu, a three-year-old girl from Bangladesh, was the last person in the world to have naturally acquired variola major and the last person in Asia to have active smallpox.
In 1977, in Somalia, Ali Maow Maalin was the last person to have naturally acquired smallpox caused by variola minor.
On September 11, 1978, Janet Parker, a medical photographer at the Birmingham University Medical School in England, was the last person to die of smallpox, which was probably acquired from the nearby Medical Microbiology Department.
In 1979, WHO recommended that all smallpox vaccination in the world cease and there was no more public vaccination beyond 1996. In 1980, smallpox was declared eradicated almost 200 years after Jenner’s discovery.
Unlike many similar contagious scourges, we were able to eradicate smallpox because it has no animal reservoir outside of humans, and the vaccine was very effective.
In late 1975, Rahima Banu, a three-year-old girl from Bangladesh, was the last person in the world to have naturally acquired variola major and the last person in Asia to have active smallpox.
In 1977, in Somalia, Ali Maow Maalin was the last person to have naturally acquired smallpox caused by variola minor.
On September 11, 1978, Janet Parker, a medical photographer at the Birmingham University Medical School in England, was the last person to die of smallpox, which was probably acquired from the nearby Medical Microbiology Department.
In 1979, WHO recommended that all smallpox vaccination in the world cease and there was no more public vaccination beyond 1996. In 1980, smallpox was declared eradicated almost 200 years after Jenner’s discovery.
Unlike many similar contagious scourges, we were able to eradicate smallpox because it has no animal reservoir outside of humans, and the vaccine was very effective.
In late 1975, Rahima Banu, a three-year-old girl from Bangladesh, was the last person in the world to have naturally acquired variola major and the last person in Asia to have active smallpox.
In 1977, in Somalia, Ali Maow Maalin was the last person to have naturally acquired smallpox caused by variola minor.
On September 11, 1978, Janet Parker, a medical photographer at the Birmingham University Medical School in England, was the last person to die of smallpox, which was probably acquired from the nearby Medical Microbiology Department.
In 1979, WHO recommended that all smallpox vaccination in the world cease and there was no more public vaccination beyond 1996. In 1980, smallpox was declared eradicated almost 200 years after Jenner’s discovery.
Unlike many similar contagious scourges, we were able to eradicate smallpox because it has no animal reservoir outside of humans, and the vaccine was very effective.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
San Francisco, California; : Buckley & Curtin, [191-] - Courtesy of the National Library of Medicine. Images from the History of Medicine (IHM), http://ihm.nlm.nih.gov/images/A21137. Public domain.
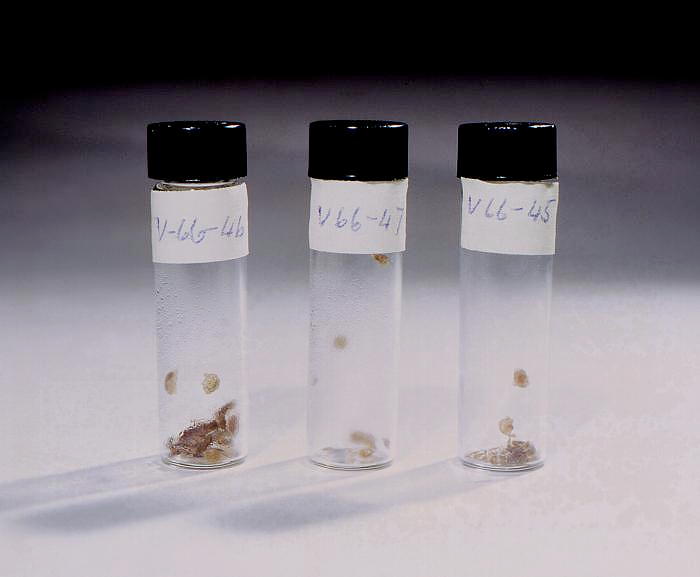
Background photo. This historic 1966 image depicts three screw-top vials, each containing crusts, or scabs, collected from smallpox patients. Public domain.
San Francisco, California; : Buckley & Curtin, [191-] - Courtesy of the National Library of Medicine. Images from the History of Medicine (IHM), http://ihm.nlm.nih.gov/images/A21137. Public domain.
Background photo. This historic 1966 image depicts three screw-top vials, each containing crusts, or scabs, collected from smallpox patients. Public domain.
San Francisco, California; : Buckley & Curtin, [191-] - Courtesy of the National Library of Medicine. Images from the History of Medicine (IHM), http://ihm.nlm.nih.gov/images/A21137. Public domain.
Background photo. This historic 1966 image depicts three screw-top vials, each containing crusts, or scabs, collected from smallpox patients. Public domain.
Unfortunately, the smallpox virus was not completely destroyed. Today, known smallpox virus exists in two places in the world; the CDC in Atlanta, Georgia, and the State Research Center of Virology and Biotechnology (VECTOR Institute) in Koltsovo, Russia. While these are high-level containment centers, we have to remember the story of Janet Parker, to understand that as long as smallpox is present anywhere, we are at risk.
Smallpox scabs like the ones in this image were once used for variolation but were also collected for study. This is very problematic and poses some genuine risks even today. In 2014, the CDC reported workers clearing out a little-used cold-storage room belonging to the Food and Drug Administration found a cardboard box containing six sealed glass tubes labeled with the scientific name for smallpox, “variola.” Two of the tubes contained viable smallpox virus for the severe strain called variola major.
Vaccination for smallpox reportedly is only good for about seven years, so the vast majority of the world today is susceptible. The official US statement is that presently there is enough vaccine to cover our population, but there is no proof of these supplies. What about the rest of the world?
As long as smallpox exists in these two labs, or in some as yet hidden sample bottles of scabs, we are at risk. The coronavirus pandemic would pale in comparison should smallpox suddenly burst back onto the world stage.
Unfortunately, the smallpox virus was not completely destroyed. Today, known smallpox virus exists in two places in the world; the CDC in Atlanta, Georgia, and the State Research Center of Virology and Biotechnology (VECTOR Institute) in Koltsovo, Russia. While these are high-level containment centers, we have to remember the story of Janet Parker, to understand that as long as smallpox is present anywhere, we are at risk.
Smallpox scabs like the ones in this image were once used for variolation but were also collected for study. This is very problematic and poses some genuine risks even today. In 2014, the CDC reported workers clearing out a little-used cold-storage room belonging to the Food and Drug Administration found a cardboard box containing six sealed glass tubes labeled with the scientific name for smallpox, “variola.” Two of the tubes contained viable smallpox virus for the severe strain called variola major.
Vaccination for smallpox reportedly is only good for about seven years, so the vast majority of the world today is susceptible. The official US statement is that presently there is enough vaccine to cover our population, but there is no proof of these supplies. What about the rest of the world?
As long as smallpox exists in these two labs, or in some as yet hidden sample bottles of scabs, we are at risk. The coronavirus pandemic would pale in comparison should smallpox suddenly burst back onto the world stage.
Unfortunately, the smallpox virus was not completely destroyed. Today, known smallpox virus exists in two places in the world; the CDC in Atlanta, Georgia, and the State Research Center of Virology and Biotechnology (VECTOR Institute) in Koltsovo, Russia. While these are high-level containment centers, we have to remember the story of Janet Parker, to understand that as long as smallpox is present anywhere, we are at risk.
Smallpox scabs like the ones in this image were once used for variolation but were also collected for study. This is very problematic and poses some genuine risks even today. In 2014, the CDC reported workers clearing out a little-used cold-storage room belonging to the Food and Drug Administration found a cardboard box containing six sealed glass tubes labeled with the scientific name for smallpox, “variola.” Two of the tubes contained viable smallpox virus for the severe strain called variola major.
Vaccination for smallpox reportedly is only good for about seven years, so the vast majority of the world today is susceptible. The official US statement is that presently there is enough vaccine to cover our population, but there is no proof of these supplies. What about the rest of the world?
As long as smallpox exists in these two labs, or in some as yet hidden sample bottles of scabs, we are at risk. The coronavirus pandemic would pale in comparison should smallpox suddenly burst back onto the world stage.
- WHO declared smallpox eradicated in 1980.
- Success in eradicating smallpox completely was possible because it only infects humans.
- Smallpox does still exist in two known places in the world: the CDC in Atlanta and the VECTOR institute in Russia.
- In 2014, vials containing infectious smallpox scab scrapings were discovered in an FDA utility room.
- The concern is that, between the virus stores at the CDC and VECTOR and as-yet-to-discovered scab vials, smallpox could once again become a worldwide killer.
- Reportedly, the CDC has enough vaccine to immunize the entire population of the United States, though immunity is probably about seven years.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
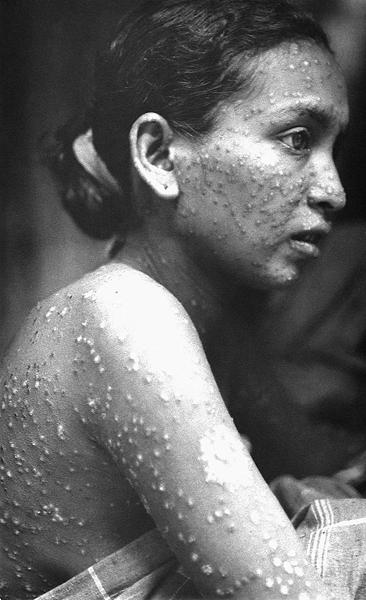

Photographed in 1975, during Bangladesh’s Smallpox Eradication Campaign, this girl who had received a prior vaccination, displayed what is referred to as a modified smallpox reaction. Modified means that the disease ran a more rapid clinical course, when compared to the evolution of ordinary-type, or unmodified smallpox. The rash evolved to crusting scabs in about 10 days, rather than the 14 days, or more, seen in ordinary smallpox. In addition, there are usually fewer lesions than with ordinary smallpox, and they may be atypical. There is also less of a fever during the rash phase. However, the prodrome, or symptoms that forewarn the onset of the frank disease, may be as severe as with ordinary smallpox. Public domain.
Photographed in 1975, during Bangladesh’s Smallpox Eradication Campaign, this girl who had received a prior vaccination, displayed what is referred to as a modified smallpox reaction. Modified means that the disease ran a more rapid clinical course, when compared to the evolution of ordinary-type, or unmodified smallpox. The rash evolved to crusting scabs in about 10 days, rather than the 14 days, or more, seen in ordinary smallpox. In addition, there are usually fewer lesions than with ordinary smallpox, and they may be atypical. There is also less of a fever during the rash phase. However, the prodrome, or symptoms that forewarn the onset of the frank disease, may be as severe as with ordinary smallpox. Public domain.
Photographed in 1975, during Bangladesh’s Smallpox Eradication Campaign, this girl who had received a prior vaccination, displayed what is referred to as a modified smallpox reaction. Modified means that the disease ran a more rapid clinical course, when compared to the evolution of ordinary-type, or unmodified smallpox. The rash evolved to crusting scabs in about 10 days, rather than the 14 days, or more, seen in ordinary smallpox. In addition, there are usually fewer lesions than with ordinary smallpox, and they may be atypical. There is also less of a fever during the rash phase. However, the prodrome, or symptoms that forewarn the onset of the frank disease, may be as severe as with ordinary smallpox. Public domain.
Unfortunately, the smallpox virus was not completely destroyed. Today, known smallpox virus exists in two places in the world; the CDC in Atlanta, Georgia, and the State Research Center of Virology and Biotechnology (VECTOR Institute) in Koltsovo, Russia. While these are high-level containment centers, we have to remember the story of Janet Parker, to understand that as long as smallpox is present anywhere, we are at risk.
Smallpox scabs like the ones in this image were once used for variolation but were also collected for study. This is very problematic and poses some genuine risks even today. In 2014, the CDC reported workers clearing out a little-used cold-storage room belonging to the Food and Drug Administration found a cardboard box containing six sealed glass tubes labeled with the scientific name for smallpox, “variola.” Two of the tubes contained viable smallpox virus for the severe strain called variola major.
Vaccination for smallpox reportedly is only good for about seven years, so the vast majority of the world today is susceptible. The official US statement is that presently there is enough vaccine to cover our population, but there is no proof of these supplies. What about the rest of the world?
As long as smallpox exists in these two labs, or in some as yet hidden sample bottles of scabs, we are at risk. The coronavirus pandemic would pale in comparison should smallpox suddenly burst back onto the world stage.
Unfortunately, the smallpox virus was not completely destroyed. Today, known smallpox virus exists in two places in the world; the CDC in Atlanta, Georgia, and the State Research Center of Virology and Biotechnology (VECTOR Institute) in Koltsovo, Russia. While these are high-level containment centers, we have to remember the story of Janet Parker, to understand that as long as smallpox is present anywhere, we are at risk.
Smallpox scabs like the ones in this image were once used for variolation but were also collected for study. This is very problematic and poses some genuine risks even today. In 2014, the CDC reported workers clearing out a little-used cold-storage room belonging to the Food and Drug Administration found a cardboard box containing six sealed glass tubes labeled with the scientific name for smallpox, “variola.” Two of the tubes contained viable smallpox virus for the severe strain called variola major.
Vaccination for smallpox reportedly is only good for about seven years, so the vast majority of the world today is susceptible. The official US statement is that presently there is enough vaccine to cover our population, but there is no proof of these supplies. What about the rest of the world?
As long as smallpox exists in these two labs, or in some as yet hidden sample bottles of scabs, we are at risk. The coronavirus pandemic would pale in comparison should smallpox suddenly burst back onto the world stage.
Often vaccine opponents’ prime argument against immunization is that it weakens or destroys the immune system. There is simply no evidence for that. We already have an innate immune system response that can react to some infectious challenges with the first exposure. That is not true of smallpox. Only those who survived the infection developed immunity.
Our immune systems have a memory for future challenges from an infectious agent and its antigens. That memory varies from a handful of years to a lifelong immunity. For most things, antigen exposure is our only real defense. Healthy immune systems thrive on antigen exposure. A few years ago, a study of three-year-olds with pica (eating dirt) showed they had healthier immune systems than children who didn’t because of antigen exposure. For that same reason, we don’t want antibiotics in our soaps since a sterile environment is actually bad for us.
Why not use antibiotics instead of vaccines to treat all infections? Antibiotics only treat bacteria, and we have a lot of different medicines for that. The more we use them, the more the bacteria develop resistance. There are bacteria now that have become so resistant that there is no known treatment. We have only very few antiviral medications, and the two possible smallpox antivirals have never been tested in humans.
- Smallpox was the largest, deadliest plague the world has ever known.
- The coincident protection of cowpox infection led to a highly effective vaccine that would eradicate smallpox.
- Opposition to vaccination has always been present since the first smallpox vaccine was created.
- As long as there are stocks of live smallpox virus in known and unknown places, the world is at risk.
- Were smallpox to get back into the wild, it would be difficult to distinguish, at least early on, from chickenpox.
- There is no good, proven treatment specific to smallpox.
- Some viruses have non-human hosts and so permanent eradication will probably not be possible.
- Vaccination for smallpox proved the value of prevention over any treatment.
- The success of smallpox vaccination is the gold standard against which we measure the prevention of all other infectious pathogens.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.


These children are lying in a Drinker respirator, also known as an iron lung, because of paralytic polio.
These children are lying in a Drinker respirator, also known as an iron lung, because of paralytic polio.
These children are lying in a Drinker respirator, also known as an iron lung, because of paralytic polio.

The success with smallpox directed our attention to polio. Polio spreads through fecal-oral contamination. It passes through the pharyngeal and intestinal mucosa. For around 72%, the infection doesn’t spread and symptoms can even be inapparent. About 24% have only minor symptoms such as fever, malaise, headache, nausea, vomiting, constipation, or sore throat.
Non-paralytic polio causes an aseptic meningitis without paralysis, but only accounts for about 4% of infections and recovery in 2 to 10 days is rapid and complete. Paralytic polio accounts for under 1% of polio, but it is devastating. In children, it begins like the usual polio infections with typical symptoms of minor illness with a symptom-free period of 1 to 3 days. Adolescents and adults seem to skip the minor illness period and have more severe pain in the affected extremities.
The virus then rapidly spreads to the spinal cord where it causes flaccid paralysis as it replicates and kills the nerve cells there. If polio spreads further to the brain, it is called bulbar poliomyelitis, which can weaken or even ablate the ability to breathe.
The paralysis is lifelong as the nerve cells don’t regenerate. Paralysis and pain can worsen after 15 to 40 years beyond the acute infection, and this is called post-polio syndrome. Oddly, post-polio syndrome is more common in females for unknown reasons.
The success with smallpox directed our attention to polio. Polio spreads through fecal-oral contamination. It passes through the pharyngeal and intestinal mucosa. For around 72%, the infection doesn’t spread and symptoms can even be inapparent. About 24% have only minor symptoms such as fever, malaise, headache, nausea, vomiting, constipation, or sore throat.
Non-paralytic polio causes an aseptic meningitis without paralysis, but only accounts for about 4% of infections and recovery in 2 to 10 days is rapid and complete. Paralytic polio accounts for under 1% of polio, but it is devastating. In children, it begins like the usual polio infections with typical symptoms of minor illness with a symptom-free period of 1 to 3 days. Adolescents and adults seem to skip the minor illness period and have more severe pain in the affected extremities.
The virus then rapidly spreads to the spinal cord where it causes flaccid paralysis as it replicates and kills the nerve cells there. If polio spreads further to the brain, it is called bulbar poliomyelitis, which can weaken or even ablate the ability to breathe.
The paralysis is lifelong as the nerve cells don’t regenerate. Paralysis and pain can worsen after 15 to 40 years beyond the acute infection, and this is called post-polio syndrome. Oddly, post-polio syndrome is more common in females for unknown reasons.
The success with smallpox directed our attention to polio. Polio spreads through fecal-oral contamination. It passes through the pharyngeal and intestinal mucosa. For around 72%, the infection doesn’t spread and symptoms can even be inapparent. About 24% have only minor symptoms such as fever, malaise, headache, nausea, vomiting, constipation, or sore throat.
Non-paralytic polio causes an aseptic meningitis without paralysis, but only accounts for about 4% of infections and recovery in 2 to 10 days is rapid and complete. Paralytic polio accounts for under 1% of polio, but it is devastating. In children, it begins like the usual polio infections with typical symptoms of minor illness with a symptom-free period of 1 to 3 days. Adolescents and adults seem to skip the minor illness period and have more severe pain in the affected extremities.
The virus then rapidly spreads to the spinal cord where it causes flaccid paralysis as it replicates and kills the nerve cells there. If polio spreads further to the brain, it is called bulbar poliomyelitis, which can weaken or even ablate the ability to breathe.
The paralysis is lifelong as the nerve cells don’t regenerate. Paralysis and pain can worsen after 15 to 40 years beyond the acute infection, and this is called post-polio syndrome. Oddly, post-polio syndrome is more common in females for unknown reasons.
- Polio, a viral illness spread through fecal contamination of water, became problematic as urbanization concentrated masses of people.
- About 1% of polio victims become paralyzed and experience great difficulty breathing.
- Iron lungs like the Drinker respirator were invented to treat respiratory paralysis which could improve within weeks or remain lifelong.
- Permanent damage could result in limb dysfunction and even confine the victim to a wheelchair.
- Post-polio pain syndrome sometimes occurred and worsened over 15 to 20 years.
- Like smallpox, polio does not affect other animals, so the hope was that a vaccine could eliminate it.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

This video is helpful in understanding why vaccines can give protection without exeriencing the full disease.
This video is helpful in understanding why vaccines can give protection without exeriencing the full disease.
This video is helpful in understanding why vaccines can give protection without exeriencing the full disease.

This video shows how the injector vaccinated Tonga preventing a mass outbreak of smallpox in 1964.
This video shows how the injector vaccinated Tonga preventing a mass outbreak of smallpox in 1964.
This video shows how the injector vaccinated Tonga preventing a mass outbreak of smallpox in 1964.
Background image. Created in 1976, this historic photograph showed an adult female receiving a vaccination that was administered by a public health clinician, by way of a jet injector, also known as a “Ped-O-Jet®”, during the nationwide Swine Flu vaccination campaign, which began October 1, 1976.
Background image. Created in 1976, this historic photograph showed an adult female receiving a vaccination that was administered by a public health clinician, by way of a jet injector, also known as a “Ped-O-Jet®”, during the nationwide Swine Flu vaccination campaign, which began October 1, 1976.
Background image. Created in 1976, this historic photograph showed an adult female receiving a vaccination that was administered by a public health clinician, by way of a jet injector, also known as a “Ped-O-Jet®”, during the nationwide Swine Flu vaccination campaign, which began October 1, 1976.
Our immune system thrives on antigen challenge! We need it to be healthy. Vaccines act like cowpox did for smallpox. They trigger a memory response without causing the disease of the infection itself.
Some vaccine opponents want to delay vaccines, but there is no valid reason for this. Infections often have variable ages at which they cause disease. Vaccine schedules are specifically timed to prevent the infection for which they are indicated.
Some opponents also want to pick and choose which vaccines they will give. That is problematic if a child is not protected against measles, though. Measles can cause the immune system to forget how to respond to infections for which it already has acquired a memory. That immune memory loss occurs regardless of whether immunity came from a previous infection or as a result of vaccination. This an immune amnesia can leave individuals with a lifelong sickly tendency.
Acquired or adaptive immunity comes from antigen exposure and accounts for the vast bulk of our immune defenses. We are constantly exposed to infectious foreign antigens, probably in the hundreds of thousands in the first year of life alone. This is important beyond infectious agents, too. Recently, it has been shown that delaying solids and breastfeeding exclusively to 9 to 12 months significantly increases the risk of food allergies.
(This video takes a deeper dive into the immune system—it will not be on the test.)
Our immune system thrives on antigen challenge! We need it to be healthy. Vaccines act like cowpox did for smallpox. They trigger a memory response without causing the disease of the infection itself.
Some vaccine opponents want to delay vaccines, but there is no valid reason for this. Infections often have variable ages at which they cause disease. Vaccine schedules are specifically timed to prevent the infection for which they are indicated.
Some opponents also want to pick and choose which vaccines they will give. That is problematic if a child is not protected against measles, though. Measles can cause the immune system to forget how to respond to infections for which it already has acquired a memory. That immune memory loss occurs regardless of whether immunity came from a previous infection or as a result of vaccination. This an immune amnesia can leave individuals with a lifelong sickly tendency.
Acquired or adaptive immunity comes from antigen exposure and accounts for the vast bulk of our immune defenses. We are constantly exposed to infectious foreign antigens, probably in the hundreds of thousands in the first year of life alone. This is important beyond infectious agents, too. Recently, it has been shown that delaying solids and breastfeeding exclusively to 9 to 12 months significantly increases the risk of food allergies.
(This video takes a deeper dive into the immune system—it will not be on the test.)
Our immune system thrives on antigen challenge! We need it to be healthy. Vaccines act like cowpox did for smallpox. They trigger a memory response without causing the disease of the infection itself.
Some vaccine opponents want to delay vaccines, but there is no valid reason for this. Infections often have variable ages at which they cause disease. Vaccine schedules are specifically timed to prevent the infection for which they are indicated.
Some opponents also want to pick and choose which vaccines they will give. That is problematic if a child is not protected against measles, though. Measles can cause the immune system to forget how to respond to infections for which it already has acquired a memory. That immune memory loss occurs regardless of whether immunity came from a previous infection or as a result of vaccination. This an immune amnesia can leave individuals with a lifelong sickly tendency.
Acquired or adaptive immunity comes from antigen exposure and accounts for the vast bulk of our immune defenses. We are constantly exposed to infectious foreign antigens, probably in the hundreds of thousands in the first year of life alone. This is important beyond infectious agents, too. Recently, it has been shown that delaying solids and breastfeeding exclusively to 9 to 12 months significantly increases the risk of food allergies.
(This video takes a deeper dive into the immune system—it will not be on the test.)
- Our bodies are exposed to hundreds of thousands of foreign protein antigens in the first years of life.
- There are two kinds of immunity against foreign proteins in viruses and bacteria: innate and acquired.
- Innate immunity is a relatively narrow ability to react to foreign proteins at the first exposure.
- Acquired immunity occurs only after the first exposure and accounts for the majority of our immune protection.
- If an initial infection occurs which inflicts serious illness, the individual may be permanently injured or even die before acquired immunity can establish resistance.
- Vaccination is the attempt to acquire immunity without causing full-blown disease, and so render us subsequently impervious.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
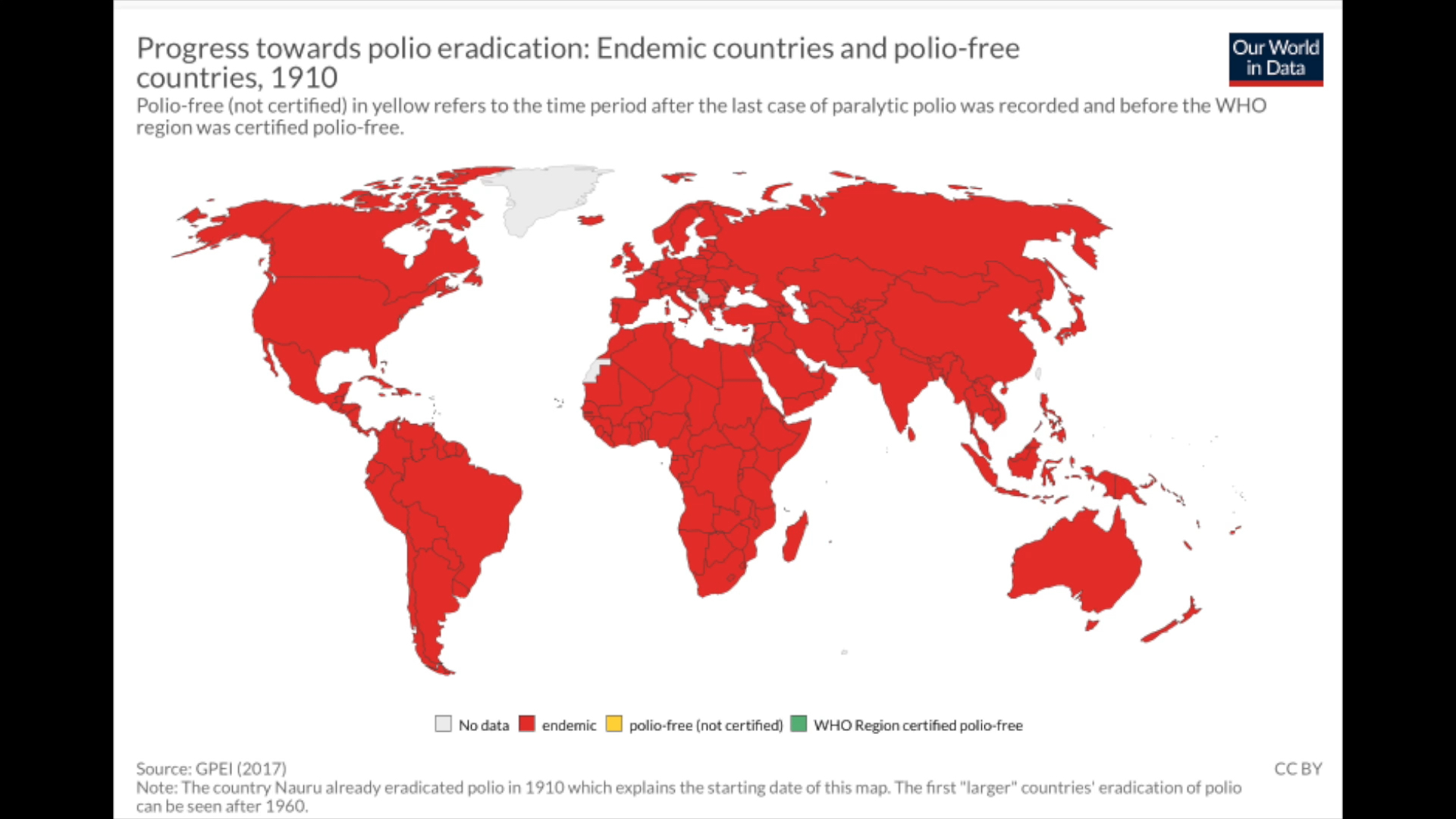
This animation showing worldwide polio vaccination over time. Red means endemic and spreading widely. Yellow means polio free, but not certified by the WHO. Green means certified polio free.
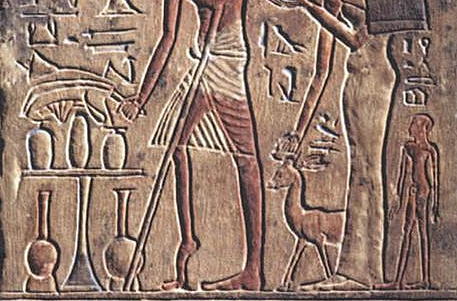
Background: Like smallpox, polio was known centuries back in history. The Egyptian stele from the 18th dynasty around 1400-1300 BC shows a man with a small, shrunken right leg in a position suggesting polio.
This animation showing worldwide polio vaccination over time. Red means endemic and spreading widely. Yellow means polio free, but not certified by the WHO. Green means certified polio free.
Background: Like smallpox, polio was known centuries back in history. The Egyptian stele from the 18th dynasty around 1400-1300 BC shows a man with a small, shrunken right leg in a position suggesting polio.
This animation showing worldwide polio vaccination over time. Red means endemic and spreading widely. Yellow means polio free, but not certified by the WHO. Green means certified polio free.
Background: Like smallpox, polio was known centuries back in history. The Egyptian stele from the 18th dynasty around 1400-1300 BC shows a man with a small, shrunken right leg in a position suggesting polio.
Once polio was confined to local endemic areas, but as the population and travel increased in the 19th and 20th centuries, it swept into epidemic proportions. Mortality rates soared with the epidemics; polio killed 27.1% of those infected in New York in 1916. Prior to vaccines, polio was the leading cause of permanent disability in children.
Two approaches to a vaccine were pursued initially. Jonas Salk developed an inactivated, dead injectable polio virus vaccine in 1955. Albert Sabin developed a live attenuated oral poliovirus vaccine in 1961. The live attenuated oral poliovirus quickly controlled polio in industrialized countries. The advantage of the attenuated oral polio vaccine is that the vaccinated individual spreads the virus to their contacts, who also become infected and immune. They then spread their attenuated poliovirus to their contacts.
The disadvantage of this is that over time, the attenuated poliovirus can regain its virulence and itself produce and spread full-blown polio, called vaccine-associated paralytic polio. The inactivated injectable polio virus doesn’t cause polio and doesn’t spread person to person. For this reason, injectable polio vaccine has been the only polio vaccine used in the US since 2000.
Once polio was confined to local endemic areas, but as the population and travel increased in the 19th and 20th centuries, it swept into epidemic proportions. Mortality rates soared with the epidemics; polio killed 27.1% of those infected in New York in 1916. Prior to vaccines, polio was the leading cause of permanent disability in children.
Two approaches to a vaccine were pursued initially. Jonas Salk developed an inactivated, dead injectable polio virus vaccine in 1955. Albert Sabin developed a live attenuated oral poliovirus vaccine in 1961. The live attenuated oral poliovirus quickly controlled polio in industrialized countries. The advantage of the attenuated oral polio vaccine is that the vaccinated individual spreads the virus to their contacts, who also become infected and immune. They then spread their attenuated poliovirus to their contacts.
The disadvantage of this is that over time, the attenuated poliovirus can regain its virulence and itself produce and spread full-blown polio, called vaccine-associated paralytic polio. The inactivated injectable polio virus doesn’t cause polio and doesn’t spread person to person. For this reason, injectable polio vaccine has been the only polio vaccine used in the US since 2000.
Once polio was confined to local endemic areas, but as the population and travel increased in the 19th and 20th centuries, it swept into epidemic proportions. Mortality rates soared with the epidemics; polio killed 27.1% of those infected in New York in 1916. Prior to vaccines, polio was the leading cause of permanent disability in children.
Two approaches to a vaccine were pursued initially. Jonas Salk developed an inactivated, dead injectable polio virus vaccine in 1955. Albert Sabin developed a live attenuated oral poliovirus vaccine in 1961. The live attenuated oral poliovirus quickly controlled polio in industrialized countries. The advantage of the attenuated oral polio vaccine is that the vaccinated individual spreads the virus to their contacts, who also become infected and immune. They then spread their attenuated poliovirus to their contacts.
The disadvantage of this is that over time, the attenuated poliovirus can regain its virulence and itself produce and spread full-blown polio, called vaccine-associated paralytic polio. The inactivated injectable polio virus doesn’t cause polio and doesn’t spread person to person. For this reason, injectable polio vaccine has been the only polio vaccine used in the US since 2000.
- Polio is a serious threat to the world because it spreads through poor sanitation.
- In the mid 1900s, there was a massive effort to develop a vaccine which led to two types; one live, but inactivated and oral, and another killed, but injectable.
- Each virus or bacteria has its own way of spreading in humans and animals which makes vaccine development specific to each.
- Polio has some similarities to smallpox, but others, like coronavirus, require different strategies.
- The live, inactivated virus vaccine could be passed passively between individuals, but then later, after passing a number of times from individual to individual, regain its virulence and cause full-blown polio.
- In the Cutter incident, the filtering step in the manufacturer's process of killing all the virus resulted in some children actually getting full-blown polio by hidden live virus.
- The vaccine production process since then is carefully scrutinized to prevent any such recurrence.
- Like smallpox, the success of polio vaccination appears to be on the brink of worldwide elimination.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Corynebacterium diphtheriae. Left: A view of a child’s upper body, focusing on her head and neck, revealing a condition referred to as bull neck. Right: Diphtheria skin lesion on a patient’s lower leg. Public domain. Center: Dirty white pseudomembrane classically seen in diphtheria. Dileepunnikri, CC BY-3.0
Corynebacterium diphtheriae. Left: A view of a child’s upper body, focusing on her head and neck, revealing a condition referred to as bull neck. Right: Diphtheria skin lesion on a patient’s lower leg. Public domain. Center: Dirty white pseudomembrane classically seen in diphtheria. Dileepunnikri, CC BY-3.0
Corynebacterium diphtheriae. Left: A view of a child’s upper body, focusing on her head and neck, revealing a condition referred to as bull neck. Right: Diphtheria skin lesion on a patient’s lower leg. Public domain. Center: Dirty white pseudomembrane classically seen in diphtheria. Dileepunnikri, CC BY-3.0
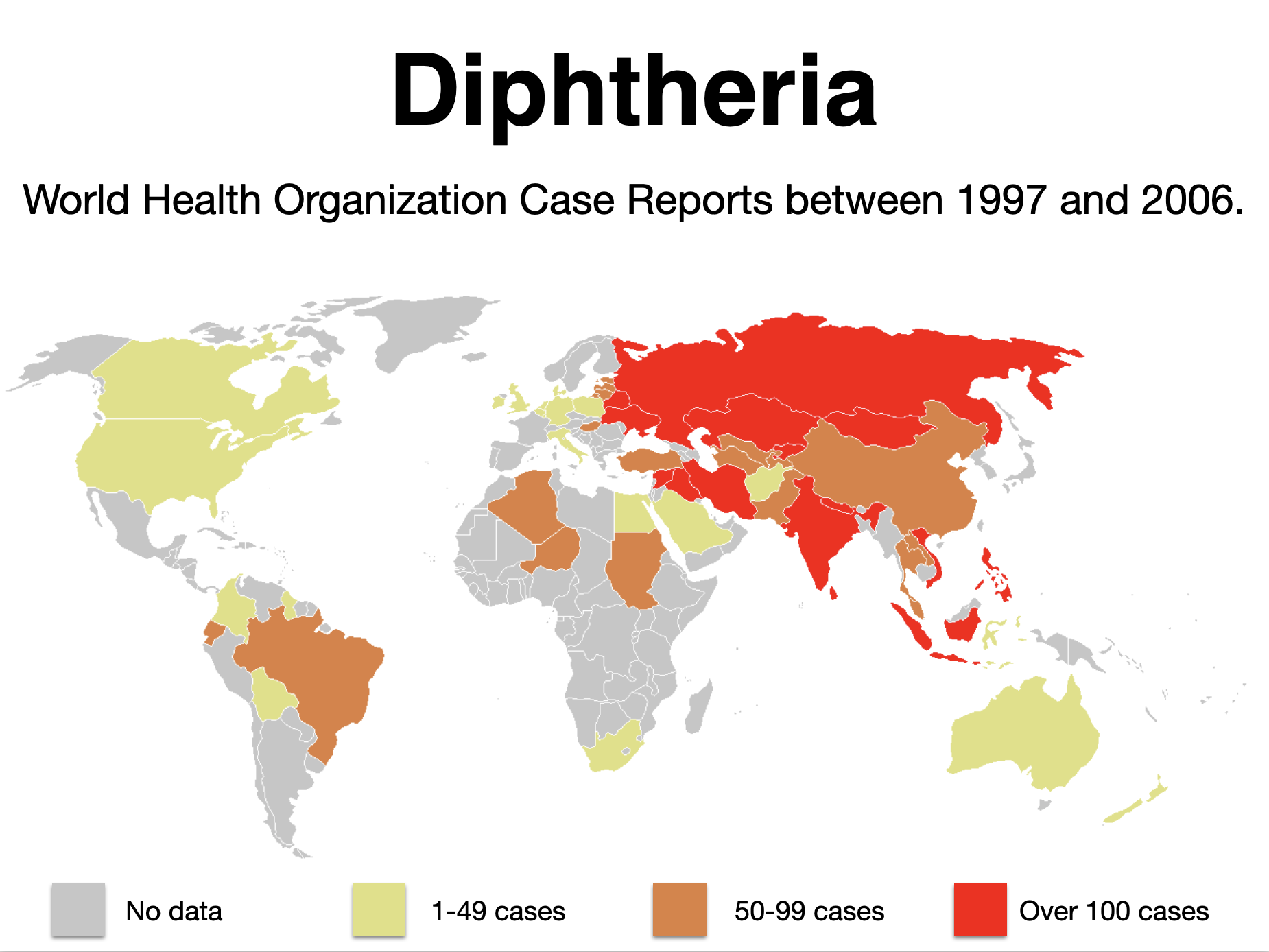
In contrast to smallpox and polio, diphtheria is still very much an infectious concern in the world. It is a bacterial illness spreads by droplet transmission to nasopharynx, larynx, and skin. A gray oropharyngeal membrane forms which can bleed and also become dislodged.
Incubation is 1 to 5 days after infection. Cutaneous diphtheria toxin destroys flesh. Nasopharyngeal carriage is common. Fever is usually not higher than 38.5°C (101.3°F), and there can be a croup-like bark. Lymph nodes in the neck can become markedly enlarged, and edema there is called a “bullneck,” is a very serious sign.
The gray pseudomembrane adheres firmly to the throat within a couple of days of infection and can slough off in pieces or as a whole. They can cause pneumonia or aspiration and suffocation.
The treatment for diphtheria is directed both at the toxin and the bacteria. Diphtheria antitoxin known as toxoid. Routine vaccination with diphtheria toxoid is very effective at prevention. We use antibiotics in patients and in carriers. They do not improve healing of the local skin infection.
In contrast to smallpox and polio, diphtheria is still very much an infectious concern in the world. It is a bacterial illness spreads by droplet transmission to nasopharynx, larynx, and skin. A gray oropharyngeal membrane forms which can bleed and also become dislodged.
Incubation is 1 to 5 days after infection. Cutaneous diphtheria toxin destroys flesh. Nasopharyngeal carriage is common. Fever is usually not higher than 38.5°C (101.3°F), and there can be a croup-like bark. Lymph nodes in the neck can become markedly enlarged, and edema there is called a “bullneck,” is a very serious sign.
The gray pseudomembrane adheres firmly to the throat within a couple of days of infection and can slough off in pieces or as a whole. They can cause pneumonia or aspiration and suffocation.
The treatment for diphtheria is directed both at the toxin and the bacteria. Diphtheria antitoxin known as toxoid. Routine vaccination with diphtheria toxoid is very effective at prevention. We use antibiotics in patients and in carriers. They do not improve healing of the local skin infection.
In contrast to smallpox and polio, diphtheria is still very much an infectious concern in the world. It is a bacterial illness spreads by droplet transmission to nasopharynx, larynx, and skin. A gray oropharyngeal membrane forms which can bleed and also become dislodged.
Incubation is 1 to 5 days after infection. Cutaneous diphtheria toxin destroys flesh. Nasopharyngeal carriage is common. Fever is usually not higher than 38.5°C (101.3°F), and there can be a croup-like bark. Lymph nodes in the neck can become markedly enlarged, and edema there is called a “bullneck,” is a very serious sign.
The gray pseudomembrane adheres firmly to the throat within a couple of days of infection and can slough off in pieces or as a whole. They can cause pneumonia or aspiration and suffocation.
The treatment for diphtheria is directed both at the toxin and the bacteria. Diphtheria antitoxin known as toxoid. Routine vaccination with diphtheria toxoid is very effective at prevention. We use antibiotics in patients and in carriers. They do not improve healing of the local skin infection.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Diphtheria and smallpox represent two different diseases, which pose similar risks because of large swaths of unvaccinated people. Until the late 1970s, billions of people worldwide received smallpox vaccine. Smallpox vaccination however is only good for about 7 years (maybe up to 10) before the immunity wanes.
From 1983 through 2002, most US service members did not get vaccinated against smallpox. Between December 2002 and May 2014, more than 2.4 million service members were vaccinated for smallpox. Smallpox vaccine is still used routinely to protect a small number of people who work in the labs with the smallpox virus.
About 95% of people are protected within 10 days after smallpox vaccination. Single dose vaccination provides substantial immunity while three doses protect for over thirty years—just the same as the yellow fever vaccine.
If vaccination percentages fall and diphtheria again breaks out, there would be a substantial shift in vaccine acceptance. However, if smallpox were to break out with its 30% mortality rate, there would be mass panic to get vaccinated.
Diphtheria vaccine is something we already have in adequate supply. Smallpox vaccine is however not available to the public. One source I found said there were enough doses of the smallpox vaccine in the US to treat “everyone who would need it.”
“Everyone who would need it” was never defined, however.
Diphtheria and smallpox represent two different diseases, which pose similar risks because of large swaths of unvaccinated people. Until the late 1970s, billions of people worldwide received smallpox vaccine. Smallpox vaccination however is only good for about 7 years (maybe up to 10) before the immunity wanes.
From 1983 through 2002, most US service members did not get vaccinated against smallpox. Between December 2002 and May 2014, more than 2.4 million service members were vaccinated for smallpox. Smallpox vaccine is still used routinely to protect a small number of people who work in the labs with the smallpox virus.
About 95% of people are protected within 10 days after smallpox vaccination. Single dose vaccination provides substantial immunity while three doses protect for over thirty years—just the same as the yellow fever vaccine.
If vaccination percentages fall and diphtheria again breaks out, there would be a substantial shift in vaccine acceptance. However, if smallpox were to break out with its 30% mortality rate, there would be mass panic to get vaccinated.
Diphtheria vaccine is something we already have in adequate supply. Smallpox vaccine is however not available to the public. One source I found said there were enough doses of the smallpox vaccine in the US to treat “everyone who would need it.”
“Everyone who would need it” was never defined, however.
Diphtheria and smallpox represent two different diseases, which pose similar risks because of large swaths of unvaccinated people. Until the late 1970s, billions of people worldwide received smallpox vaccine. Smallpox vaccination however is only good for about 7 years (maybe up to 10) before the immunity wanes.
From 1983 through 2002, most US service members did not get vaccinated against smallpox. Between December 2002 and May 2014, more than 2.4 million service members were vaccinated for smallpox. Smallpox vaccine is still used routinely to protect a small number of people who work in the labs with the smallpox virus.
About 95% of people are protected within 10 days after smallpox vaccination. Single dose vaccination provides substantial immunity while three doses protect for over thirty years—just the same as the yellow fever vaccine.
If vaccination percentages fall and diphtheria again breaks out, there would be a substantial shift in vaccine acceptance. However, if smallpox were to break out with its 30% mortality rate, there would be mass panic to get vaccinated.
Diphtheria vaccine is something we already have in adequate supply. Smallpox vaccine is however not available to the public. One source I found said there were enough doses of the smallpox vaccine in the US to treat “everyone who would need it.”
“Everyone who would need it” was never defined, however.
- Diphtheria is a serious bacterial illness that can produce a gray pseudomembrane in the throat which can cause suffocation if it is dislodged.
- Additionally, it produces a toxin which can cause serious skin and soft tissue damage similar to the flesh-eating bacteria.
- Diphtheria vaccine produces immunity which targets both the bacteria and the toxin, hence it is know as toxoid vaccine.
- The history of Nome, Alaska, where vaccine stocks ran out just as the winter closed in, underscored the role that vaccines play in the prevention of disease.
- While smallpox virus is not a threat in the wild at present, diphtheria bacteria is an ongoing threat.
- If vaccination rates fall, diphtheria will come back because the bacterium is present in soil, water, plant matter, and food products; it therefore cannot be eradicated once and for like smallpox.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
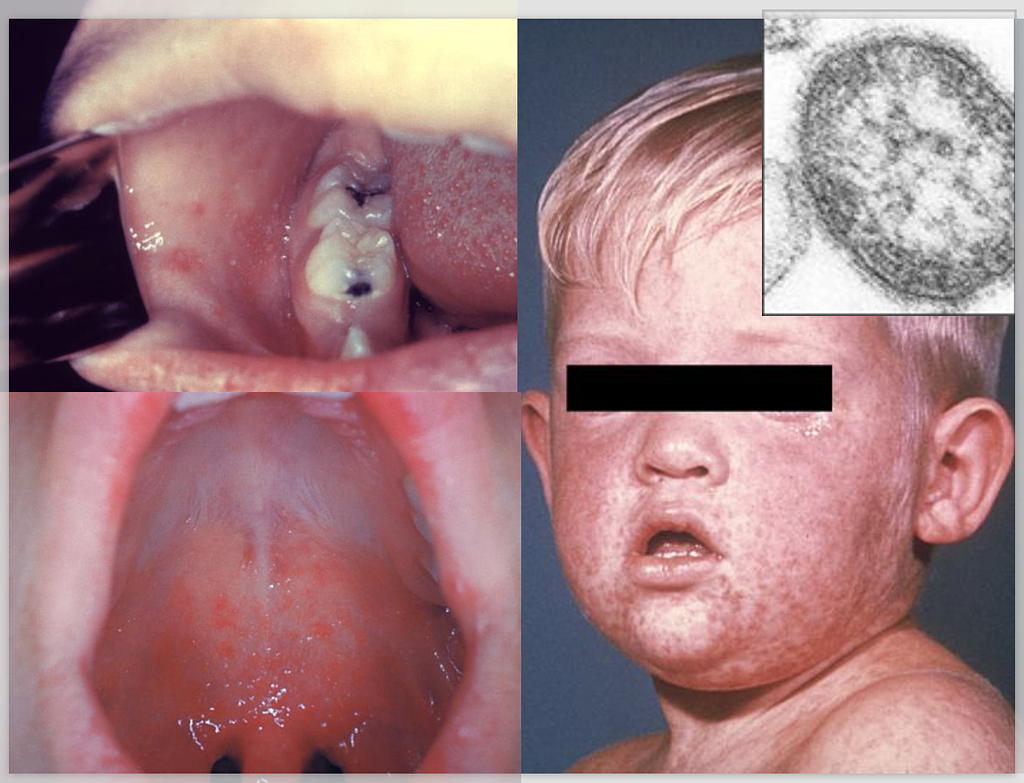
“Koplik spots” on the mucosa of the cheeks and tongue, which appear as irregularly-shaped, bright red spots often with a bluish-white central dot. Right: The face of a young boy with measles, which was captured on the third day of its characteristic rash. Public domain.
“Koplik spots” on the mucosa of the cheeks and tongue, which appear as irregularly-shaped, bright red spots often with a bluish-white central dot. Right: The face of a young boy with measles, which was captured on the third day of its characteristic rash. Public domain.
Top left: The third pre-eruptive day with “Koplik spots” indicative of the beginning onset of measles. In the prodromal or beginning stages, one of the signs of the onset of measles is the eruption of “Koplik spots” on the mucosa of the cheeks and tongue, which appear as irregularly-shaped, bright red spots often with a bluish-white central dot. Right: The face of a young boy with measles, which was captured on the third day of its characteristic rash. Public domain.
Measles is a highly contagious, paramyxovirus, of the genus Morbillivirus. The onset of symptoms is about 7 to 14 days after exposure and includes high fever, cough, runny nose known as coryza, red, watery conjunctivitis without crusting, a characteristic pharyngeal rash around day two, and a general macular to maculopapular rash around day four which often is associated with a temperature in the 104°F range.
The pharyngeal rash develops with Koplik spots that are white, salt-like bumps within the wide area of inflammation. It only lasts for one to two days though, so it is often gone before clinicians could see it on exam. Infected individuals are contagious from up to 4 to 5 days before symptoms arise. What is the big deal today about measles?
Measles is a highly contagious, paramyxovirus, of the genus Morbillivirus. The onset of symptoms is about 7 to 14 days after exposure and includes high fever, cough, runny nose known as coryza, red, watery conjunctivitis without crusting, a characteristic pharyngeal rash around day two, and a general macular to maculopapular rash around day four which often is associated with a temperature in the 104°F range.
The pharyngeal rash develops with Koplik spots that are white, salt-like bumps within the wide area of inflammation. It only lasts for one to two days though, so it is often gone before clinicians could see it on exam. Infected individuals are contagious from up to 4 to 5 days before symptoms arise. What is the big deal today about measles?
Measles is a highly contagious, paramyxovirus, of the genus Morbillivirus. The onset of symptoms is about 7 to 14 days after exposure and includes high fever, cough, runny nose known as coryza, red, watery conjunctivitis without crusting, a characteristic pharyngeal rash around day two, and a general macular to maculopapular rash around day four which often is associated with a temperature in the 104°F range.
The pharyngeal rash develops with Koplik spots that are white, salt-like bumps within the wide area of inflammation. It only lasts for one to two days though, so it is often gone before clinicians could see it on exam. Infected individuals are contagious from up to 4 to 5 days before symptoms arise. What is the big deal today about measles?

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
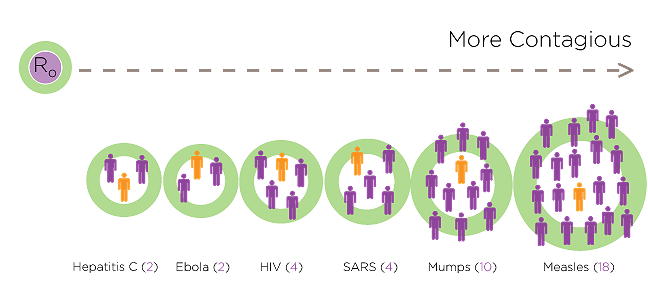
We characterize the contagion of a disease by its R0 (R naught) factor where a population has no immunity. It is a measure of how many people an index case is likely to infect. The Spanish flu that killed 50 million in 1917-1918 had an R0 of 1.4 to 2.8. The R0 for SARS-CoV-2 was first estimated to be 2 to 4, but it is closer to that of the flu.
Measles on the other hand has an R0 of around 12 to 18. Contagion from one person is much more likely to others. But that is not the whole story. The virus can linger in the air for up to two or three hours after an infected person has left an exam room or waiting area. If thirty susceptible individuals are exposed in those areas during that time then 27 of them will become infected.
Negative feelings about vaccines have led to significant drops in measles vaccination in recent years. Where there are pockets of groups of people who have little or no immunity, measles will run rampant. The high risk of measles contagion fuels a growing political movement against those refusing to vaccinate for measles in particular. Our personal rights are clashing against mandates suggesting the public good.
The financial risk of contagion is pervasive. Medical office liability is a part of why you are seeing more and more offices refusing to accept unvaccinated children as patients. State governments like Georgia have moved to protect businesses from any customer liability in the SARS-CoV-2 pandemic for the same reason.
We characterize the contagion of a disease by its R0 (R naught) factor where a population has no immunity. It is a measure of how many people an index case is likely to infect. The Spanish flu that killed 50 million in 1917-1918 had an R0 of 1.4 to 2.8. The R0 for SARS-CoV-2 was first estimated to be 2 to 4, but it is closer to that of the flu.
Measles on the other hand has an R0 of around 12 to 18. Contagion from one person is much more likely to others. But that is not the whole story. The virus can linger in the air for up to two or three hours after an infected person has left an exam room or waiting area. If thirty susceptible individuals are exposed in those areas during that time then 27 of them will become infected.
Negative feelings about vaccines have led to significant drops in measles vaccination in recent years. Where there are pockets of groups of people who have little or no immunity, measles will run rampant. The high risk of measles contagion fuels a growing political movement against those refusing to vaccinate for measles in particular. Our personal rights are clashing against mandates suggesting the public good.
The financial risk of contagion is pervasive. Medical office liability is a part of why you are seeing more and more offices refusing to accept unvaccinated children as patients. State governments like Georgia have moved to protect businesses from any customer liability in the SARS-CoV-2 pandemic for the same reason.
We characterize the contagion of a disease by its R0 (R naught) factor where a population has no immunity. It is a measure of how many people an index case is likely to infect. The Spanish flu that killed 50 million in 1917-1918 had an R0 of 1.4 to 2.8. The R0 for SARS-CoV-2 was first estimated to be 2 to 4, but it is closer to that of the flu.
Measles on the other hand has an R0 of around 12 to 18. Contagion from one person is much more likely to others. But that is not the whole story. The virus can linger in the air for up to two or three hours after an infected person has left an exam room or waiting area. If thirty susceptible individuals are exposed in those areas during that time then 27 of them will become infected.
Negative feelings about vaccines have led to significant drops in measles vaccination in recent years. Where there are pockets of groups of people who have little or no immunity, measles will run rampant. The high risk of measles contagion fuels a growing political movement against those refusing to vaccinate for measles in particular. Our personal rights are clashing against mandates suggesting the public good.
The financial risk of contagion is pervasive. Medical office liability is a part of why you are seeing more and more offices refusing to accept unvaccinated children as patients. State governments like Georgia have moved to protect businesses from any customer liability in the SARS-CoV-2 pandemic for the same reason.
- Measles is a virus that causes serious and sometimes fatal illness (subacute pansclerosing encephalitis) in children and adults.
- It is more serious because it can also permanently damage the immune system so that it "forgets" the immunity already established to other infectious agents; we call this immune amnesia.
- The virus is present only in humans.
- It is one of the most highly contagious viruses, and it is passed by droplets into the air where it lingers for two or three hours.
- Vaccination worldwide could eliminate this virus just as vaccination did for smallpox.
- Opposition to measles vaccination along with pockets of populations with poor vaccine access have prevented measles eradication once and for all.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
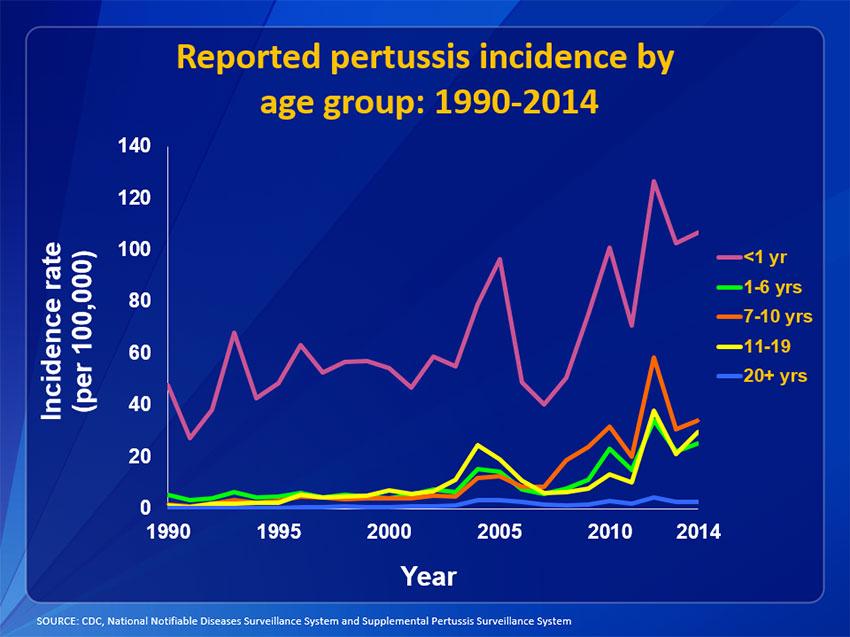
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Above are the bacteria magnified under a microscope. Bordetella pertussis bacteria cause pertussis disease.
Credit: CDC
Above are the bacteria magnified under a microscope. Bordetella pertussis bacteria cause pertussis disease.
Credit: CDC
Above are the bacteria magnified under a microscope. Bordetella pertussis bacteria cause pertussis disease.
Credit: CDC
Whooping cough, or pertussis, is just as much a problem today as it was for me over thirty years ago when I started practice. To accurately diagnose it then and even today, a calcium alginate swab is inserted deep into the post-nasal area in an attempt to collect cuboidal epithelial cells mucous membranes. The swab is then rolled onto a glass slide where those cells will hopefully be transferred. It is then air dried and transported in a protective cardboard slide holder.
The lab treats the slide with a specific fluorescent antibody which lights up whooping cough bacteria stuck onto those epithelial cells under the microscope. Despite some newer blood tests, there is still not a better way to test for Pertussis in my opinion.
Vaccination does not always imply immunity to Pertussis. Improvements in the vaccine of thirty years ago have made the pertussis vaccine and all other vaccines safe. Febrile reactions essentially vanished. Newer studies have shown that even in the rare case of febrile reactions and even febrile seizures that occur within the first day of any vaccination do not cause neurologic damage.
An adult who has a cough last three weeks or so has a 21% chance of actually having pertussis, even if they were vaccinated as a child. Among children who are diagnosed with whooping cough, 35% of the time they were infected by their mothers.
That is the reason you are seeing more and more obstetricians vaccinating expectant mothers during pregnancy. The optimal time for this is around 30 weeks gestation. The antibodies that she develops will be passed on across the placenta and her newborn will retain those pertussis antibodies for three or even four months. That is the most critical time to prevent whooping cough since the mortality is highest at that age.
Many ERs, urgent cares, and physicians offices have shifted from Td (tetanus toxoid) to Tdap which includes acellurlar pertussis. That gives adults a pertussis booster which is important, since adults are the repository for the bacteria which infects children.
Whooping cough, or pertussis, is just as much a problem today as it was for me over thirty years ago when I started practice. To accurately diagnose it then and even today, a calcium alginate swab is inserted deep into the post-nasal area in an attempt to collect cuboidal epithelial cells mucous membranes. The swab is then rolled onto a glass slide where those cells will hopefully be transferred. It is then air dried and transported in a protective cardboard slide holder.
The lab treats the slide with a specific fluorescent antibody which lights up whooping cough bacteria stuck onto those epithelial cells under the microscope. Despite some newer blood tests, there is still not a better way to test for Pertussis in my opinion.
Vaccination does not always imply immunity to Pertussis. Improvements in the vaccine of thirty years ago have made the pertussis vaccine and all other vaccines safe. Febrile reactions essentially vanished. Newer studies have shown that even in the rare case of febrile reactions and even febrile seizures that occur within the first day of any vaccination do not cause neurologic damage.
An adult who has a cough last three weeks or so has a 21% chance of actually having pertussis, even if they were vaccinated as a child. Among children who are diagnosed with whooping cough, 35% of the time they were infected by their mothers.
That is the reason you are seeing more and more obstetricians vaccinating expectant mothers during pregnancy. The optimal time for this is around 30 weeks gestation. The antibodies that she develops will be passed on across the placenta and her newborn will retain those pertussis antibodies for three or even four months. That is the most critical time to prevent whooping cough since the mortality is highest at that age.
Many ERs, urgent cares, and physicians offices have shifted from Td (tetanus toxoid) to Tdap which includes acellurlar pertussis. That gives adults a pertussis booster which is important, since adults are the repository for the bacteria which infects children.
Whooping cough, or pertussis, is just as much a problem today as it was for me over thirty years ago when I started practice. To accurately diagnose it then and even today, a calcium alginate swab is inserted deep into the post-nasal area in an attempt to collect cuboidal epithelial cells mucous membranes. The swab is then rolled onto a glass slide where those cells will hopefully be transferred. It is then air dried and transported in a protective cardboard slide holder.
The lab treats the slide with a specific fluorescent antibody which lights up whooping cough bacteria stuck onto those epithelial cells under the microscope. Despite some newer blood tests, there is still not a better way to test for Pertussis in my opinion.
Vaccination does not always imply immunity to Pertussis. Improvements in the vaccine of thirty years ago have made the pertussis vaccine and all other vaccines safe. Febrile reactions essentially vanished. Newer studies have shown that even in the rare case of febrile reactions and even febrile seizures that occur within the first day of any vaccination do not cause neurologic damage.
An adult who has a cough last three weeks or so has a 21% chance of actually having pertussis, even if they were vaccinated as a child. Among children who are diagnosed with whooping cough, 35% of the time they were infected by their mothers.
That is the reason you are seeing more and more obstetricians vaccinating expectant mothers during pregnancy. The optimal time for this is around 30 weeks gestation. The antibodies that she develops will be passed on across the placenta and her newborn will retain those pertussis antibodies for three or even four months. That is the most critical time to prevent whooping cough since the mortality is highest at that age.
Many ERs, urgent cares, and physicians offices have shifted from Td (tetanus toxoid) to Tdap which includes acellurlar pertussis. That gives adults a pertussis booster which is important, since adults are the repository for the bacteria which infects children.
- Bordetella pertussis is a bacteria found exclusively in humans and known commonly as the “hundred days cough.”
- It causes a severe upper respiratory tract infection that produces a prolonged, paroxysmal, and exasperating cough.
- In babies especially, the characteristic “whooping” cough can be so severe that the lack of oxygen causes death.
- The primary reservoir promoting continued propagation of infection are infected adults who go undiagnosed.
- Because adults go undiagnosed, infants and very young children are at risk.
- This bacteria theoretically could be eradicated except that it often goes undiagnosed in the adult reservoir.
- Treatment will eradicate the bacteria while the cough can remain for many weeks; thus regular vaccination will likely be required for the foreseeable future.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
- Infectious disease poses the greatest threat to the world as population increases and individuals are compacted in closer and closer proximity.
- Smallpox, in particular, demonstrates that treatment, which is often a primary focus for the the public, is really secondary to the protection from a properly armed immune system.
- Vaccination offers a cheaper solution than treatment solutions.
- There are many diseases we have not discussed which need to be, and are being, addressed with vaccine prevention.
- So what are the arguments being presented against vaccination?
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Background image. Compulsory vaccination in New Jersey in the 1880s. Creator: National Library of Medicine
Background image. Compulsory vaccination in New Jersey in the 1880s. Creator: National Library of Medicine
Background image. Compulsory vaccination in New Jersey in the 1880s. Creator: National Library of Medicine
Despite these improvements and demonstrated vaccine safety, government vaccination mandates for public schools are why we have the National VICP (Vaccine Injury Compensation Program). This program is a no-fault claim resource that is important liability protection for medical providers. Without this program, each medical practice could (and would) be sued to the point that any and all medical care would cease due to the financial burden of defending such suits.
Even physicians who oppose vaccination could be sued for injury related to infectious disease for which there was a prevention by non-vaxxing parents who later changed their minds. The VICP programs is not only the core reason why we can even have the choice to vaccinate or not, but the very foundation that pediatricians can really give care to children at all.
Today, physicians have to also be concerned that they can be sued for disease occurrence due to NOT vaccinating children, even when parents have knowingly refused vaccines. That has fostered the move by many physicians to refuse to accept children whose parents refuse vaccines.
It has to be understood that the VICP would NOT cover physicians in that case. I suspect this will become more and more the norm. Our feeling is that parents need to get all the information that we have so they can make a fully conscious decision and physicians can provide care reducing their risk of "wrongful disease," as you might call it.
Despite these improvements and demonstrated vaccine safety, government vaccination mandates for public schools are why we have the National VICP (Vaccine Injury Compensation Program). This program is a no-fault claim resource that is important liability protection for medical providers. Without this program, each medical practice could (and would) be sued to the point that any and all medical care would cease due to the financial burden of defending such suits.
Even physicians who oppose vaccination could be sued for injury related to infectious disease for which there was a prevention by non-vaxxing parents who later changed their minds. The VICP programs is not only the core reason why we can even have the choice to vaccinate or not, but the very foundation that pediatricians can really give care to children at all.
Today, physicians have to also be concerned that they can be sued for disease occurrence due to NOT vaccinating children, even when parents have knowingly refused vaccines. That has fostered the move by many physicians to refuse to accept children whose parents refuse vaccines.
It has to be understood that the VICP would NOT cover physicians in that case. I suspect this will become more and more the norm. Our feeling is that parents need to get all the information that we have so they can make a fully conscious decision and physicians can provide care reducing their risk of "wrongful disease," as you might call it.
Despite these improvements and demonstrated vaccine safety, government vaccination mandates for public schools are why we have the National VICP (Vaccine Injury Compensation Program). This program is a no-fault claim resource that is important liability protection for medical providers. Without this program, each medical practice could (and would) be sued to the point that any and all medical care would cease due to the financial burden of defending such suits.
Even physicians who oppose vaccination could be sued for injury related to infectious disease for which there was a prevention by non-vaxxing parents who later changed their minds. The VICP programs is not only the core reason why we can even have the choice to vaccinate or not, but the very foundation that pediatricians can really give care to children at all.
Today, physicians have to also be concerned that they can be sued for disease occurrence due to NOT vaccinating children, even when parents have knowingly refused vaccines. That has fostered the move by many physicians to refuse to accept children whose parents refuse vaccines.
It has to be understood that the VICP would NOT cover physicians in that case. I suspect this will become more and more the norm. Our feeling is that parents need to get all the information that we have so they can make a fully conscious decision and physicians can provide care reducing their risk of "wrongful disease," as you might call it.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Acute otitis media.
Acute otitis media.
Acute otitis media.
When I started practice in 1986, I would see one or two cases of Hemophilus influenza type b meningitis a year. Since the vaccine came out and was required for public Georgia schools, I have seen no cases since 2000. Reactions to the H. flu vaccine are nil because of all we learned with Pertussis vaccine manufacture.
H. flu vaccine was first required in Georgia in 2000.
Thirty-five years ago, 30% of ear infections were bacterial, and Streptococcus pneumoniae accounted for 30% of those. Ear infections were the bread and butter of pediatrics when I started, but not anymore since the newer vaccine for it. Pneumococcus is the prime cause of bacterial pneumonia and bacteremia. It accounted for about 20% or more of childhood fevers in my first practice but now only about 5% or less.
The take-home about these vaccines is timing. Delaying these vaccines simply opens the window to the infection rates I used to see, because that is when children are most susceptible to these pathogens. Delaying vaccines don't have any effect on improved safety and would be analogous to trying to get liability insurance for your vehicle after you have already had the wreck.
When I started practice in 1986, I would see one or two cases of Hemophilus influenza type b meningitis a year. Since the vaccine came out and was required for public Georgia schools, I have seen no cases since 2000. Reactions to the H. flu vaccine are nil because of all we learned with Pertussis vaccine manufacture.
H. flu vaccine was first required in Georgia in 2000.
Thirty-five years ago, 30% of ear infections were bacterial, and Streptococcus pneumoniae accounted for 30% of those. Ear infections were the bread and butter of pediatrics when I started, but not anymore since the newer vaccine for it. Pneumococcus is the prime cause of bacterial pneumonia and bacteremia. It accounted for about 20% or more of childhood fevers in my first practice but now only about 5% or less.
The take-home about these vaccines is timing. Delaying these vaccines simply opens the window to the infection rates I used to see, because that is when children are most susceptible to these pathogens. Delaying vaccines don't have any effect on improved safety and would be analogous to trying to get liability insurance for your vehicle after you have already had the wreck.
When I started practice in 1986, I would see one or two cases of Hemophilus influenza type b meningitis a year. Since the vaccine came out and was required for public Georgia schools, I have seen no cases since 2000. Reactions to the H. flu vaccine are nil because of all we learned with Pertussis vaccine manufacture.
H. flu vaccine was first required in Georgia in 2000.
Thirty-five years ago, 30% of ear infections were bacterial, and Streptococcus pneumoniae accounted for 30% of those. Ear infections were the bread and butter of pediatrics when I started, but not anymore since the newer vaccine for it. Pneumococcus is the prime cause of bacterial pneumonia and bacteremia. It accounted for about 20% or more of childhood fevers in my first practice but now only about 5% or less.
The take-home about these vaccines is timing. Delaying these vaccines simply opens the window to the infection rates I used to see, because that is when children are most susceptible to these pathogens. Delaying vaccines don't have any effect on improved safety and would be analogous to trying to get liability insurance for your vehicle after you have already had the wreck.
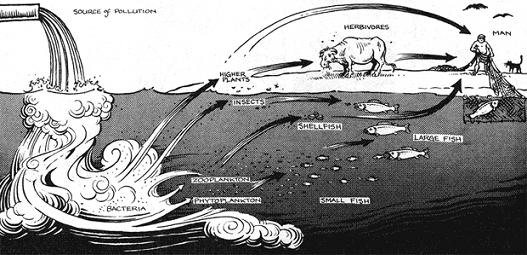
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Thimerosal, or thimersol, is a vaccine preservative that contains a very, very small amount of mercury. Multi-dose vaccine vials required a preservative to prevent bacterial contamination from repeated re-entry even with sterile injection needles. Today, almost all vaccines come in unit dose vials that don’t require this.
The concern over mercury came from an illness called Minimata Disease. Minimata Bay in Japan is a vital source of fish which is a large part of the local population’s regular diet there. As industry around the bay proliferated the water became contaminated with local industrial mercury waste. Heavy metal neuropathy caused by mercury is a devastating neurologic illness in both children and adults, and was the cause of the outcry against Thimerasol.
What most people don't understand is that there are two kinds of mercury; ethyl mercury and methyl mercury. Methyl mercury is what is present in industrial wastes and is the cause of Minimata disease. It has a half-life of 49 days and accumulates dramatically in fish exposed to these industrial waste.
Thimerosal, which contains just over 49% mercury by weight, is metabolized to ethyl mercury and thiosalicylate. Ethyl mercury only has a half-life of 3 days. You would never inject thimerosal as shown in this image, but the quantity in each vial is miniscule. That means that mercury given now only in multi-dose vials presents absolutely no risk at all. Still opponents continue to bring up this issue.
Thimerosal, or thimersol, is a vaccine preservative that contains a very, very small amount of mercury. Multi-dose vaccine vials required a preservative to prevent bacterial contamination from repeated re-entry even with sterile injection needles. Today, almost all vaccines come in unit dose vials that don’t require this.
The concern over mercury came from an illness called Minimata Disease. Minimata Bay in Japan is a vital source of fish which is a large part of the local population’s regular diet there. As industry around the bay proliferated the water became contaminated with local industrial mercury waste. Heavy metal neuropathy caused by mercury is a devastating neurologic illness in both children and adults, and was the cause of the outcry against Thimerasol.
What most people don't understand is that there are two kinds of mercury; ethyl mercury and methyl mercury. Methyl mercury is what is present in industrial wastes and is the cause of Minimata disease. It has a half-life of 49 days and accumulates dramatically in fish exposed to these industrial waste.
Thimerosal, which contains just over 49% mercury by weight, is metabolized to ethyl mercury and thiosalicylate. Ethyl mercury only has a half-life of 3 days. You would never inject thimerosal as shown in this image, but the quantity in each vial is miniscule. That means that mercury given now only in multi-dose vials presents absolutely no risk at all. Still opponents continue to bring up this issue.
Thimerosal, or thimersol, is a vaccine preservative that contains a very, very small amount of mercury. Multi-dose vaccine vials required a preservative to prevent bacterial contamination from repeated re-entry even with sterile injection needles. Today, almost all vaccines come in unit dose vials that don’t require this.
The concern over mercury came from an illness called Minimata Disease. Minimata Bay in Japan is a vital source of fish which is a large part of the local population’s regular diet there. As industry around the bay proliferated the water became contaminated with local industrial mercury waste. Heavy metal neuropathy caused by mercury is a devastating neurologic illness in both children and adults, and was the cause of the outcry against Thimerasol.
What most people don't understand is that there are two kinds of mercury; ethyl mercury and methyl mercury. Methyl mercury is what is present in industrial wastes and is the cause of Minimata disease. It has a half-life of 49 days and accumulates dramatically in fish exposed to these industrial waste.
Thimerosal, which contains just over 49% mercury by weight, is metabolized to ethyl mercury and thiosalicylate. Ethyl mercury only has a half-life of 3 days. You would never inject thimerosal as shown in this image, but the quantity in each vial is miniscule. That means that mercury given now only in multi-dose vials presents absolutely no risk at all. Still opponents continue to bring up this issue.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Formaldehyde molecule.
Formaldehyde molecule.
Formaldehyde molecule.
Formaldehyde is used to attenuate vaccines that have a live virus constituent. Killing the virus and bacteria prevents infection and full blown disease. The NIH guidelines specify allowable formaldehyde residual in vaccines. For Diphtheria, levels cannot be more than 0.02% which equals 0.1mg per 0.5ml dose (with formaldehyde density of 0.815g/ml).
The EPA sets standards for acceptable oral reference dose, or RfD, of formaldehyde. RfD is defined as “an estimate (with uncertainty spanning perhaps an order of magnitude) of a continuous inhalation exposure or a daily exposure to the human population (including sensitive subgroups) that is likely to be without an appreciable risk of deleterious non-cancer effects during a lifetime.” The RfD for formaldehyde (oral administration) is 0.2 mg/kg of bodyweight per day. For a 22 pound (or 10 kg) child, that calculates to an acceptable level of exposure at or below 2 mg daily for a prolonged period.
Comparatively, vaccine formaldehyde for the entire first year of recommended vaccines is well below the daily acceptable EPA exposure levels.
Further to this, formaldehyde is naturally present in our own body as a result of normal biochemical processes. Our body contains around 2.6 mg/L of formaldehyde. A 22 pound (10 kg) child is around 65% to 75% water which means their body consists of 6.5 kg of water. Because water is 1ml/gm, that means this child has 6.5 liters of water in their body. That means they have as a baseline 16.9 mg of formaldehyde at all times.
Any vaccine dose containing 0.1mg of formaldehyde has 169 times less formaldehyde than is already present in their body. Additionally we must consider what ways are we exposed to formaldehyde in our daily lives especially in the furniture in our homes.
Formaldehyde is used to attenuate vaccines that have a live virus constituent. Killing the virus and bacteria prevents infection and full blown disease. The NIH guidelines specify allowable formaldehyde residual in vaccines. For Diphtheria, levels cannot be more than 0.02% which equals 0.1mg per 0.5ml dose (with formaldehyde density of 0.815g/ml).
The EPA sets standards for acceptable oral reference dose, or RfD, of formaldehyde. RfD is defined as “an estimate (with uncertainty spanning perhaps an order of magnitude) of a continuous inhalation exposure or a daily exposure to the human population (including sensitive subgroups) that is likely to be without an appreciable risk of deleterious non-cancer effects during a lifetime.” The RfD for formaldehyde (oral administration) is 0.2 mg/kg of bodyweight per day. For a 22 pound (or 10 kg) child, that calculates to an acceptable level of exposure at or below 2 mg daily for a prolonged period.
Comparatively, vaccine formaldehyde for the entire first year of recommended vaccines is well below the daily acceptable EPA exposure levels.
Further to this, formaldehyde is naturally present in our own body as a result of normal biochemical processes. Our body contains around 2.6 mg/L of formaldehyde. A 22 pound (10 kg) child is around 65% to 75% water which means their body consists of 6.5 kg of water. Because water is 1ml/gm, that means this child has 6.5 liters of water in their body. That means they have as a baseline 16.9 mg of formaldehyde at all times.
Any vaccine dose containing 0.1mg of formaldehyde has 169 times less formaldehyde than is already present in their body. Additionally we must consider what ways are we exposed to formaldehyde in our daily lives especially in the furniture in our homes.
Formaldehyde is used to attenuate vaccines that have a live virus constituent. Killing the virus and bacteria prevents infection and full blown disease. The NIH guidelines specify allowable formaldehyde residual in vaccines. For Diphtheria, levels cannot be more than 0.02% which equals 0.1mg per 0.5ml dose (with formaldehyde density of 0.815g/ml).
The EPA sets standards for acceptable oral reference dose, or RfD, of formaldehyde. RfD is defined as “an estimate (with uncertainty spanning perhaps an order of magnitude) of a continuous inhalation exposure or a daily exposure to the human population (including sensitive subgroups) that is likely to be without an appreciable risk of deleterious non-cancer effects during a lifetime.” The RfD for formaldehyde (oral administration) is 0.2 mg/kg of bodyweight per day. For a 22 pound (or 10 kg) child, that calculates to an acceptable level of exposure at or below 2 mg daily for a prolonged period.
Comparatively, vaccine formaldehyde for the entire first year of recommended vaccines is well below the daily acceptable EPA exposure levels.
Further to this, formaldehyde is naturally present in our own body as a result of normal biochemical processes. Our body contains around 2.6 mg/L of formaldehyde. A 22 pound (10 kg) child is around 65% to 75% water which means their body consists of 6.5 kg of water. Because water is 1ml/gm, that means this child has 6.5 liters of water in their body. That means they have as a baseline 16.9 mg of formaldehyde at all times.
Any vaccine dose containing 0.1mg of formaldehyde has 169 times less formaldehyde than is already present in their body. Additionally we must consider what ways are we exposed to formaldehyde in our daily lives especially in the furniture in our homes.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
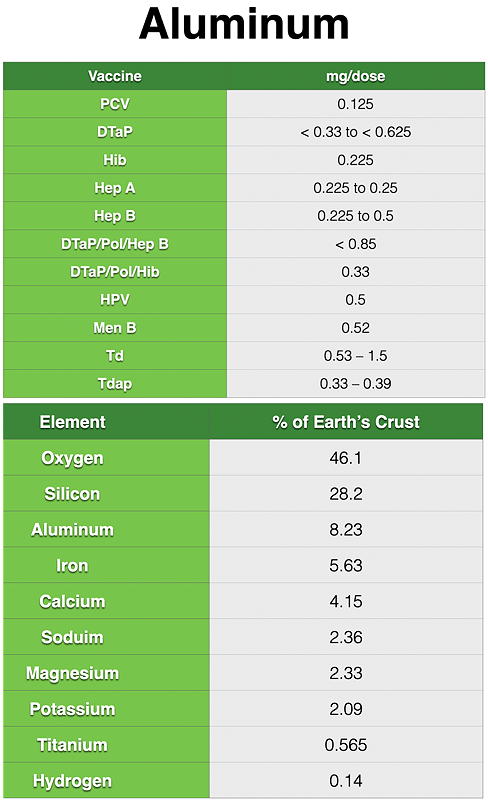
Aluminum is valuable in non-live vaccines because it is an adjuvant, which means it boosts the immune response of vaccines. Adjuvants reduce the amount of vaccine required to produce immunogenic response.
Adults consume about 7 to 9 mg of aluminum a day. In the first six months of life, non-soy formula-fed babies consume about 38 mg. Breastfed infants get 7 mg in the first six months. Babies fed soy formula get 117 mg.
By comparison, infants get about 4.4 mg of aluminum in their regular vaccines in the first six months, albeit through injection rather than ingestion.
Aluminum is the most abundant metal constituting 8% of the earth’s crust. We are all exposed to aluminum all day every day. If you eliminated aluminum from vaccines, you wouldn’t reduce the total daily aluminum exposure by any degree. Aluminum toxicity is therefore also a non-issue in vaccines while being giving the take rates at lower injection doses a boost.
Vaccine opponents usually reach for aluminum as a last ditch effort to sway public opinion.
Aluminum is valuable in non-live vaccines because it is an adjuvant, which means it boosts the immune response of vaccines. Adjuvants reduce the amount of vaccine required to produce immunogenic response.
Adults consume about 7 to 9 mg of aluminum a day. In the first six months of life, non-soy formula-fed babies consume about 38 mg. Breastfed infants get 7 mg in the first six months. Babies fed soy formula get 117 mg.
By comparison, infants get about 4.4 mg of aluminum in their regular vaccines in the first six months, albeit through injection rather than ingestion.
Aluminum is the most abundant metal constituting 8% of the earth’s crust. We are all exposed to aluminum all day every day. If you eliminated aluminum from vaccines, you wouldn’t reduce the total daily aluminum exposure by any degree. Aluminum toxicity is therefore also a non-issue in vaccines while being giving the take rates at lower injection doses a boost.
Vaccine opponents usually reach for aluminum as a last ditch effort to sway public opinion.
Aluminum is valuable in non-live vaccines because it is an adjuvant, which means it boosts the immune response of vaccines. Adjuvants reduce the amount of vaccine required to produce immunogenic response.
Adults consume about 7 to 9 mg of aluminum a day. In the first six months of life, non-soy formula-fed babies consume about 38 mg. Breastfed infants get 7 mg in the first six months. Babies fed soy formula get 117 mg.
By comparison, infants get about 4.4 mg of aluminum in their regular vaccines in the first six months, albeit through injection rather than ingestion.
Aluminum is the most abundant metal constituting 8% of the earth’s crust. We are all exposed to aluminum all day every day. If you eliminated aluminum from vaccines, you wouldn’t reduce the total daily aluminum exposure by any degree. Aluminum toxicity is therefore also a non-issue in vaccines while being giving the take rates at lower injection doses a boost.
Vaccine opponents usually reach for aluminum as a last ditch effort to sway public opinion.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
A common concern is that there are so many things now in one vaccine which surely must be harmful. Mistakenly thinking it is safer, parents often ask me to do an altered schedule, and thus spread vaccines out instead of grouping them according the published guidelines.
It has been shown that grouping immunizations improves the immunogenic take rate for each individual vaccine. Tdap is one such combination vaccine that I hope will completely replace the Td because it also has acellular pertussis in it.
If mothers are vaccinated with Tdap prior to pregnancy then the transplacental antibodies give passive immunity for pertussis (whooping cough) to their babies for the first three or four months. We also use Td to prevent lockjaw when someone gets a puncture with a rusty nail.
In one study that I read a few years ago, if an adult has a persistent cough for two to three weeks, the probability that pertussis was the source was around 21%. Because the repository of pertussis is in the adult population, by switching entirely from Td to Tdap, every time someone gets a Tetanus shot, we boost their immunity to pertussis and lower the risk to children.
A common concern is that there are so many things now in one vaccine which surely must be harmful. Mistakenly thinking it is safer, parents often ask me to do an altered schedule, and thus spread vaccines out instead of grouping them according the published guidelines.
It has been shown that grouping immunizations improves the immunogenic take rate for each individual vaccine. Tdap is one such combination vaccine that I hope will completely replace the Td because it also has acellular pertussis in it.
If mothers are vaccinated with Tdap prior to pregnancy then the transplacental antibodies give passive immunity for pertussis (whooping cough) to their babies for the first three or four months. We also use Td to prevent lockjaw when someone gets a puncture with a rusty nail.
In one study that I read a few years ago, if an adult has a persistent cough for two to three weeks, the probability that pertussis was the source was around 21%. Because the repository of pertussis is in the adult population, by switching entirely from Td to Tdap, every time someone gets a Tetanus shot, we boost their immunity to pertussis and lower the risk to children.
A common concern is that there are so many things now in one vaccine which surely must be harmful. Mistakenly thinking it is safer, parents often ask me to do an altered schedule, and thus spread vaccines out instead of grouping them according the published guidelines.
It has been shown that grouping immunizations improves the immunogenic take rate for each individual vaccine. Tdap is one such combination vaccine that I hope will completely replace the Td because it also has acellular pertussis in it.
If mothers are vaccinated with Tdap prior to pregnancy then the transplacental antibodies give passive immunity for pertussis (whooping cough) to their babies for the first three or four months. We also use Td to prevent lockjaw when someone gets a puncture with a rusty nail.
In one study that I read a few years ago, if an adult has a persistent cough for two to three weeks, the probability that pertussis was the source was around 21%. Because the repository of pertussis is in the adult population, by switching entirely from Td to Tdap, every time someone gets a Tetanus shot, we boost their immunity to pertussis and lower the risk to children.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Wakefield’s original study claiming that MMR was the cause of autism included just 12 children. Initially it made me cringe when it was first published because I knew the value of vaccines. This claim had to be seriously considered because it alleged specifically that a serious medical illness in children was caused by vaccination.
While the Lancet, in 2010, declared Andrew Wakefield’s original 1998 study a fraud, the damage was done. Wakefield profited greatly from the litigation where as an expert witness he based everything on his own article. Wakefield had also filed a UK patent application for his own vaccine/therapeutic agent for measles and inflammatory bowel disease in June 1997, several months before he published his MMR/autism article.
He was kicked out of Britain and practiced in Austin, Texas for about a year before getting out of medicine altogether so I last heard. He continues to fuel the anti vaccine movement even today despite being discredited.
It is primarily because of this article that I spend so much time on vaccine education. We had better remember Welch and his outbreak of diphtheria. We need to keep in mind that Smallpox virus still exists in known and unknown places in the world and it may not be “if” but “when” it sneaks out of hiding.
Wakefield’s original study claiming that MMR was the cause of autism included just 12 children. Initially it made me cringe when it was first published because I knew the value of vaccines. This claim had to be seriously considered because it alleged specifically that a serious medical illness in children was caused by vaccination.
While the Lancet, in 2010, declared Andrew Wakefield’s original 1998 study a fraud, the damage was done. Wakefield profited greatly from the litigation where as an expert witness he based everything on his own article. Wakefield had also filed a UK patent application for his own vaccine/therapeutic agent for measles and inflammatory bowel disease in June 1997, several months before he published his MMR/autism article.
He was kicked out of Britain and practiced in Austin, Texas for about a year before getting out of medicine altogether so I last heard. He continues to fuel the anti vaccine movement even today despite being discredited.
It is primarily because of this article that I spend so much time on vaccine education. We had better remember Welch and his outbreak of diphtheria. We need to keep in mind that Smallpox virus still exists in known and unknown places in the world and it may not be “if” but “when” it sneaks out of hiding.
Wakefield’s original study claiming that MMR was the cause of autism included just 12 children. Initially it made me cringe when it was first published because I knew the value of vaccines. This claim had to be seriously considered because it alleged specifically that a serious medical illness in children was caused by vaccination.
While the Lancet, in 2010, declared Andrew Wakefield’s original 1998 study a fraud, the damage was done. Wakefield profited greatly from the litigation where as an expert witness he based everything on his own article. Wakefield had also filed a UK patent application for his own vaccine/therapeutic agent for measles and inflammatory bowel disease in June 1997, several months before he published his MMR/autism article.
He was kicked out of Britain and practiced in Austin, Texas for about a year before getting out of medicine altogether so I last heard. He continues to fuel the anti vaccine movement even today despite being discredited.
It is primarily because of this article that I spend so much time on vaccine education. We had better remember Welch and his outbreak of diphtheria. We need to keep in mind that Smallpox virus still exists in known and unknown places in the world and it may not be “if” but “when” it sneaks out of hiding.
- The National Vaccine Injury Program (VICP) is not intended to cover up vaccine problems, but to provide a speedy recourse to those within specific guidelines, who have a possibly valid claim, and to sidestep the delay inherent in court litigation. Without the VICP, court litigation would essentially stop all vaccination.
- Government vaccine mandates are a part of medical vaccine history and are often a political football.
- For each infectious agent, vaccination timing is specific to the age of susceptibility; delaying vaccines leaves children unprotected.
- Multidose vials, fairly uncommon today, prevent bacterial contamination of vials as they are reentered with fresh syringes.
- Formaldehyde kills deadly virus so that vaccines are safe from live virus contamination.
- Aluminum, a vaccine adjuvant additive, enables smaller amounts of vaccine to produce equivalent protection of larger amounts.
- Combining vaccines in single injections is preferable because it promotes higher individual component take rates.
- The MMR and autism association was proven to be a fraud engineered by Andrew Wakefield for his financial gain.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.

The most serious claim that vaccine opponents make is that the injected materials contain aborted fetal material. This is not true, but few know or understand how this claim came to be. It started with the polio vaccines.
The Salk Polio injectable vaccine came from inactivated, or killed, polio virus. The Sabin Polio oral polio vaccine was manufactured from attenuated, or live, polio virus which had been treated with formaldehyde. The “Cutter Incident” refers to the first manufacture of the Salk version of the polio vaccine where the filters allowed some of the virus to “hide” from the formaldehyde and thus remain viable and virulent. There were children that were affected with polio.
The “Cutter Incident” initiated the first government oversight of all vaccine manufacture, and was part of the reason the National Childhood Vaccine Injury Act was passed in 1986. It created the National Vaccine Injury Compensation Program (VICP), a no-fault route for children or adults pursuing reimbursement for vaccine injury claims. It is government trust fund financed by an excise tax on all vaccines. The goal was to reduce the time for patients and their families to receive compensation through usual legal channels.
The most serious claim that vaccine opponents make is that the injected materials contain aborted fetal material. This is not true, but few know or understand how this claim came to be. It started with the polio vaccines.
The Salk Polio injectable vaccine came from inactivated, or killed, polio virus. The Sabin Polio oral polio vaccine was manufactured from attenuated, or live, polio virus which had been treated with formaldehyde. The “Cutter Incident” refers to the first manufacture of the Salk version of the polio vaccine where the filters allowed some of the virus to “hide” from the formaldehyde and thus remain viable and virulent. There were children that were affected with polio.
The “Cutter Incident” initiated the first government oversight of all vaccine manufacture, and was part of the reason the National Childhood Vaccine Injury Act was passed in 1986. It created the National Vaccine Injury Compensation Program (VICP), a no-fault route for children or adults pursuing reimbursement for vaccine injury claims. It is government trust fund financed by an excise tax on all vaccines. The goal was to reduce the time for patients and their families to receive compensation through usual legal channels.
The most serious claim that vaccine opponents make is that the injected materials contain aborted fetal material. This is not true, but few know or understand how this claim came to be. It started with the polio vaccines.
The Salk Polio injectable vaccine came from inactivated, or killed, polio virus. The Sabin Polio oral polio vaccine was manufactured from attenuated, or live, polio virus which had been treated with formaldehyde. The “Cutter Incident” refers to the first manufacture of the Salk version of the polio vaccine where the filters allowed some of the virus to “hide” from the formaldehyde and thus remain viable and virulent. There were children that were affected with polio.
The “Cutter Incident” initiated the first government oversight of all vaccine manufacture, and was part of the reason the National Childhood Vaccine Injury Act was passed in 1986. It created the National Vaccine Injury Compensation Program (VICP), a no-fault route for children or adults pursuing reimbursement for vaccine injury claims. It is government trust fund financed by an excise tax on all vaccines. The goal was to reduce the time for patients and their families to receive compensation through usual legal channels.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Viral vaccine manufacture requires a continuing supply of the target virus which, unlike bacteria, do not grow outside of a host cell. The virus must take over the host cell biochemical machinery just as it would in the wild. The host cell dies, and is not included in any vaccine material. Only the virus is used to make the vaccine.
Originally monkey cell strains were used to create these viral stocks. It was discovered however that SV40 (Simian Virus 40) which did not cause disease in humans was discovered in some of these monkey host cells. As a result, the FDA decided that no human vaccines could be made using non-human cell strains.
The terms cell line and cell strains are different. Cell lines are immortalized in that they can continue to replicate indefinitely. The most famous is the HeLa cell line which came from cervical cancer cells of Henrietta Lacks who passed away from her disease, and who by the way never gave her permission for their use. It is because they are mutated cancer cells that these cell lines never die. The FDA has also refused to allow vaccines where the virus supply comes from such cells.
The proof of effectiveness had already been shown before the monkey virus was found. With these limitations, a new source of human diploid cells had to be found. These cells would not replicate forever however like a cell line.
Viral vaccine manufacture requires a continuing supply of the target virus which, unlike bacteria, do not grow outside of a host cell. The virus must take over the host cell biochemical machinery just as it would in the wild. The host cell dies, and is not included in any vaccine material. Only the virus is used to make the vaccine.
Originally monkey cell strains were used to create these viral stocks. It was discovered however that SV40 (Simian Virus 40) which did not cause disease in humans was discovered in some of these monkey host cells. As a result, the FDA decided that no human vaccines could be made using non-human cell strains.
The terms cell line and cell strains are different. Cell lines are immortalized in that they can continue to replicate indefinitely. The most famous is the HeLa cell line which came from cervical cancer cells of Henrietta Lacks who passed away from her disease, and who by the way never gave her permission for their use. It is because they are mutated cancer cells that these cell lines never die. The FDA has also refused to allow vaccines where the virus supply comes from such cells.
The proof of effectiveness had already been shown before the monkey virus was found. With these limitations, a new source of human diploid cells had to be found. These cells would not replicate forever however like a cell line.
Viral vaccine manufacture requires a continuing supply of the target virus which, unlike bacteria, do not grow outside of a host cell. The virus must take over the host cell biochemical machinery just as it would in the wild. The host cell dies, and is not included in any vaccine material. Only the virus is used to make the vaccine.
Originally monkey cell strains were used to create these viral stocks. It was discovered however that SV40 (Simian Virus 40) which did not cause disease in humans was discovered in some of these monkey host cells. As a result, the FDA decided that no human vaccines could be made using non-human cell strains.
The terms cell line and cell strains are different. Cell lines are immortalized in that they can continue to replicate indefinitely. The most famous is the HeLa cell line which came from cervical cancer cells of Henrietta Lacks who passed away from her disease, and who by the way never gave her permission for their use. It is because they are mutated cancer cells that these cell lines never die. The FDA has also refused to allow vaccines where the virus supply comes from such cells.
The proof of effectiveness had already been shown before the monkey virus was found. With these limitations, a new source of human diploid cells had to be found. These cells would not replicate forever however like a cell line.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Humans and all animals constantly shed normal cells, mostly from skin. These shed cells, however, will not grow virus. In 1961, Dr. Hayflick, working at the Wistar Institute on the campus of the University of Pennsylvania in Philadelphia, developed the WI-38 cell strain which could replicate poliovirus. Philadelphia was also experiencing a polio epidemic.
The source of the original WI-38 cell strain came from the lung tissue cells of one fetus. That is the reason some people object to vaccines, even though none of them contain fetal cells or fetal material.
Abortion was illegal in the United States at that time, so fetal tissue was provided by Dr. Sven Gard of the Karolinska Institute Medical School in Stockholm, Sweden. A family in Sweden, who felt they already had too many children, had sadly chosen to abort. Both parents were alive and well and married to each other. Dr. Gard chose their unborn child because it had no history of familial disease or cancer.
I cannot say how profoundly emotional it is for me thinking about this child. But it is certain that these parents had already chosen abortion for no reason related to any interest in their baby’s tissues. While the cell strain came from one cell of that one aborted fetus, vaccines do not contain any aborted fetal tissue material no matter what opponents try to say.
Humans and all animals constantly shed normal cells, mostly from skin. These shed cells, however, will not grow virus. In 1961, Dr. Hayflick, working at the Wistar Institute on the campus of the University of Pennsylvania in Philadelphia, developed the WI-38 cell strain which could replicate poliovirus. Philadelphia was also experiencing a polio epidemic.
The source of the original WI-38 cell strain came from the lung tissue cells of one fetus. That is the reason some people object to vaccines, even though none of them contain fetal cells or fetal material.
Abortion was illegal in the United States at that time, so fetal tissue was provided by Dr. Sven Gard of the Karolinska Institute Medical School in Stockholm, Sweden. A family in Sweden, who felt they already had too many children, had sadly chosen to abort. Both parents were alive and well and married to each other. Dr. Gard chose their unborn child because it had no history of familial disease or cancer.
I cannot say how profoundly emotional it is for me thinking about this child. But it is certain that these parents had already chosen abortion for no reason related to any interest in their baby’s tissues. While the cell strain came from one cell of that one aborted fetus, vaccines do not contain any aborted fetal tissue material no matter what opponents try to say.
Humans and all animals constantly shed normal cells, mostly from skin. These shed cells, however, will not grow virus. In 1961, Dr. Hayflick, working at the Wistar Institute on the campus of the University of Pennsylvania in Philadelphia, developed the WI-38 cell strain which could replicate poliovirus. Philadelphia was also experiencing a polio epidemic.
The source of the original WI-38 cell strain came from the lung tissue cells of one fetus. That is the reason some people object to vaccines, even though none of them contain fetal cells or fetal material.
Abortion was illegal in the United States at that time, so fetal tissue was provided by Dr. Sven Gard of the Karolinska Institute Medical School in Stockholm, Sweden. A family in Sweden, who felt they already had too many children, had sadly chosen to abort. Both parents were alive and well and married to each other. Dr. Gard chose their unborn child because it had no history of familial disease or cancer.
I cannot say how profoundly emotional it is for me thinking about this child. But it is certain that these parents had already chosen abortion for no reason related to any interest in their baby’s tissues. While the cell strain came from one cell of that one aborted fetus, vaccines do not contain any aborted fetal tissue material no matter what opponents try to say.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Neither, I, my colleagues, nor Storybook Pediatrics as a practice, endorse abortion, nor would we use use vaccines that contained material from any abortions.
While we decry that baby’s parents’ decision, we have mixed emotions. It makes me think about a heart transplant where someone besides the donor makes all the decisions. How many people die naturally or unnaturally, do so without donating tissues or cells that could help someone living.
That baby’s life mattered, and I will always remember how many people’s lives were saved as a result. Researchers have estimated vaccines made from virus which was cultivated in WI-38 secondary cell strains have prevented nearly 11 million deaths and prevented (or treated, in the example of rabies) and 4.5 billion cases of disease.
Unlike abnormal cancer cells, the WI-38 strain cultures are nearing the end of their ability to replicate. My thought is that future technology will use non-fetal stem cells to provide new cell strains. We have that technology I believe.
Today these vaccines are the ones I know that use human diploid (normal) cell strains for virus production.
• Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
• Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
• Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
• Zoster (shingles) vaccine [Zostavax/Merck]
• Adenovirus Type 4 and Type 7 oral vaccine [Barr Labs] *
• Rabies vaccine [IMOVAX/Sanofi Pasteur] *
Neither, I, my colleagues, nor Storybook Pediatrics as a practice, endorse abortion, nor would we use use vaccines that contained material from any abortions.
While we decry that baby’s parents’ decision, we have mixed emotions. It makes me think about a heart transplant where someone besides the donor makes all the decisions. How many people die naturally or unnaturally, do so without donating tissues or cells that could help someone living.
That baby’s life mattered, and I will always remember how many people’s lives were saved as a result. Researchers have estimated vaccines made from virus which was cultivated in WI-38 secondary cell strains have prevented nearly 11 million deaths and prevented (or treated, in the example of rabies) and 4.5 billion cases of disease.
Unlike abnormal cancer cells, the WI-38 strain cultures are nearing the end of their ability to replicate. My thought is that future technology will use non-fetal stem cells to provide new cell strains. We have that technology I believe.
Today these vaccines are the ones I know that use human diploid (normal) cell strains for virus production.
• Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
• Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
• Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
• Zoster (shingles) vaccine [Zostavax/Merck]
• Adenovirus Type 4 and Type 7 oral vaccine [Barr Labs] *
• Rabies vaccine [IMOVAX/Sanofi Pasteur] *
Neither, I, my colleagues, nor Storybook Pediatrics as a practice, endorse abortion, nor would we use use vaccines that contained material from any abortions.
While we decry that baby’s parents’ decision, we have mixed emotions. It makes me think about a heart transplant where someone besides the donor makes all the decisions. How many people die naturally or unnaturally, do so without donating tissues or cells that could help someone living.
That baby’s life mattered, and I will always remember how many people’s lives were saved as a result. Researchers have estimated vaccines made from virus which was cultivated in WI-38 secondary cell strains have prevented nearly 11 million deaths and prevented (or treated, in the example of rabies) and 4.5 billion cases of disease.
Unlike abnormal cancer cells, the WI-38 strain cultures are nearing the end of their ability to replicate. My thought is that future technology will use non-fetal stem cells to provide new cell strains. We have that technology I believe.
Today these vaccines are the ones I know that use human diploid (normal) cell strains for virus production.
• Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
• Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
• Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
• Zoster (shingles) vaccine [Zostavax/Merck]
• Adenovirus Type 4 and Type 7 oral vaccine [Barr Labs] *
• Rabies vaccine [IMOVAX/Sanofi Pasteur] *
Neither, I, my colleagues, nor Storybook Pediatrics as a practice, endorse abortion, nor would we use use vaccines that contained material from any abortions.
While we decry that baby’s parents’ decision, we have mixed emotions. It makes me think about a heart transplant where someone besides the donor makes all the decisions. How many people die naturally or unnaturally, do so without donating tissues or cells that could help someone living.
That baby’s life mattered, and I will always remember how many people’s lives were saved as a result. Researchers have estimated vaccines made from virus which was cultivated in WI-38 secondary cell strains have prevented nearly 11 million deaths and prevented (or treated, in the example of rabies) and 4.5 billion cases of disease.
Unlike abnormal cancer cells, the WI-38 strain cultures are nearing the end of their ability to replicate. My thought is that future technology will use non-fetal stem cells to provide new cell strains. We have that technology I believe.
Today these vaccines are the ones I know that use human diploid (normal) cell strains for virus production.
• Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
• Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
• Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
• Zoster (shingles) vaccine [Zostavax/Merck]
• Adenovirus Type 4 and Type 7 oral vaccine [Barr Labs] *
• Rabies vaccine [IMOVAX/Sanofi Pasteur] *
Neither, I, my colleagues, nor Storybook Pediatrics as a practice, endorse abortion, nor would we use use vaccines that contained material from any abortions.
While we decry that baby’s parents’ decision, we have mixed emotions. It makes me think about a heart transplant where someone besides the donor makes all the decisions. How many people die naturally or unnaturally, do so without donating tissues or cells that could help someone living.
That baby’s life mattered, and I will always remember how many people’s lives were saved as a result. Researchers have estimated vaccines made from virus which was cultivated in WI-38 secondary cell strains have prevented nearly 11 million deaths and prevented (or treated, in the example of rabies) and 4.5 billion cases of disease.
Unlike abnormal cancer cells, the WI-38 strain cultures are nearing the end of their ability to replicate. My thought is that future technology will use non-fetal stem cells to provide new cell strains. We have that technology I believe.
Today these vaccines are the ones I know that use human diploid (normal) cell strains for virus production.
• Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
• Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
• Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
• Zoster (shingles) vaccine [Zostavax/Merck]
• Adenovirus Type 4 and Type 7 oral vaccine [Barr Labs] *
• Rabies vaccine [IMOVAX/Sanofi Pasteur] *
• Hepatitis A vaccines [VAQTA/Merck, Havrix/GlaxoSmithKline, and part of Twinrix/GlaxoSmithKline]
• Rubella vaccine [MERUVAX II/Merck, part of MMR II/Merck, and ProQuad/Merck]
• Varicella (chickenpox) vaccine [Varivax/Merck, and part of ProQuad/Merck]
• Zoster (shingles) vaccine [Zostavax/Merck]
• Adenovirus Type 4 and Type 7 oral vaccine [Barr Labs] *
• Rabies vaccine [IMOVAX/Sanofi Pasteur] *
- Abortion is abhorrent. It is not true that aborted fetal tissues are added to vaccines—ever.
- Cell lines, such as HELA from Henrietta Lacks, are immortal, replicate forever, and are derived from cancer cells which have damaged DNA by default.
- Cell strains are normal cells taken from normal tissues which have a limited number of replications and so are not immortal.
- The WI-38 cell strain originated from a fibroblast cell that was taken from a Swedish child whose parents had already chosen to abort and were not (as far as is known) sought out to abort for that purpose.
- Cells are not the same as tissues and are shed in the millions from our bodies every day.
- Live virus has historically been required to create vaccines.
- The WI-38 cell strains infected with a virus result in large quantities of virus, but the WI-38 cells themselves are not used in the vaccine itself.
- The WI-38 line is about at the end of its ability to replicate; newer mRNA technology will improve both the quality and production speed of vaccines.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
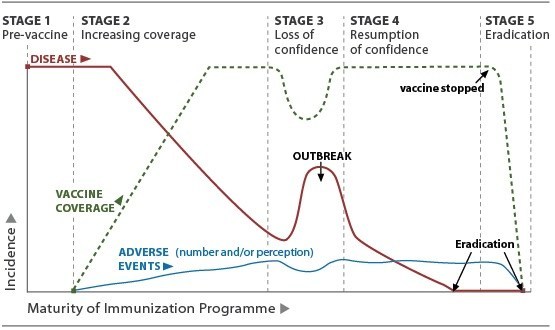
Image from World Health Organization
Image from World Health Organization
Image from World Health Organization
The graph shows the typical progression of disease with a vaccine that shows historically the public response over time.
Farwick Collinsworth and his family owned a large portion of the small Texas town. When the smallpox epidemic came, the illness took his 11-year-old granddaughter first. Next, it claimed the lives of his wife and two sons. Following them, two more grandchildren and a nephew died from the viral disease.
Around the time the small, 45-year-old Texas town was founded, the vaccine had already been available for over forty years. The widespread outbreak continued.
Four years later, in March, a riot would occur in another relatively nearby Texas town protesting a quarantine and vaccination order for the disease. The Texas governor sent the Texas Rangers led by Captain J. H. Rogers to enforce the health officials’ vaccination order more vigorously than some city’s residents thought proper. Milling protestors pelted the rangers and health care workers with harsh words and hard rocks, causing minor injuries.
The next day when Captain Rogers got word someone had telephoned a local hardware store to order 2,000 rounds of buckshot, he ordered his men to begin a house-to-house search of the area of town where the order had originated. The situation deteriorated into a riot, and after it was over, the Rangers had killed two citizens and wounded 10 others. It wasn’t until the cavalry from nearby Fort Mcintosh arrived that order was restored, and the inoculation and fumigation program continued.
The quarantine and vaccination program that began in March 1 finally ended on May 1. That first city was Plano, Texas. The protests in the second city are known as the Laredo Smallpox Riot.
The graph shows the typical progression of disease with a vaccine that shows historically the public response over time.
Farwick Collinsworth and his family owned a large portion of the small Texas town. When the smallpox epidemic came, the illness took his 11-year-old granddaughter first. Next, it claimed the lives of his wife and two sons. Following them, two more grandchildren and a nephew died from the viral disease.
Around the time the small, 45-year-old Texas town was founded, the vaccine had already been available for over forty years. The widespread outbreak continued.
Four years later, in March, a riot would occur in another relatively nearby Texas town protesting a quarantine and vaccination order for the disease. The Texas governor sent the Texas Rangers led by Captain J. H. Rogers to enforce the health officials’ vaccination order more vigorously than some city’s residents thought proper. Milling protestors pelted the rangers and health care workers with harsh words and hard rocks, causing minor injuries.
The next day when Captain Rogers got word someone had telephoned a local hardware store to order 2,000 rounds of buckshot, he ordered his men to begin a house-to-house search of the area of town where the order had originated. The situation deteriorated into a riot, and after it was over, the Rangers had killed two citizens and wounded 10 others. It wasn’t until the cavalry from nearby Fort Mcintosh arrived that order was restored, and the inoculation and fumigation program continued.
The quarantine and vaccination program that began in March 1 finally ended on May 1. That first city was Plano, Texas. The protests in the second city are known as the Laredo Smallpox Riot.
The graph shows the typical progression of disease with a vaccine that shows historically the public response over time.
Farwick Collinsworth and his family owned a large portion of the small Texas town. When the smallpox epidemic came, the illness took his 11-year-old granddaughter first. Next, it claimed the lives of his wife and two sons. Following them, two more grandchildren and a nephew died from the viral disease.
Around the time the small, 45-year-old Texas town was founded, the vaccine had already been available for over forty years. The widespread outbreak continued.
Four years later, in March, a riot would occur in another relatively nearby Texas town protesting a quarantine and vaccination order for the disease. The Texas governor sent the Texas Rangers led by Captain J. H. Rogers to enforce the health officials’ vaccination order more vigorously than some city’s residents thought proper. Milling protestors pelted the rangers and health care workers with harsh words and hard rocks, causing minor injuries.
The next day when Captain Rogers got word someone had telephoned a local hardware store to order 2,000 rounds of buckshot, he ordered his men to begin a house-to-house search of the area of town where the order had originated. The situation deteriorated into a riot, and after it was over, the Rangers had killed two citizens and wounded 10 others. It wasn’t until the cavalry from nearby Fort Mcintosh arrived that order was restored, and the inoculation and fumigation program continued.
The quarantine and vaccination program that began in March 1 finally ended on May 1. That first city was Plano, Texas. The protests in the second city are known as the Laredo Smallpox Riot.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Image from World Health Organization
Image from World Health Organization
Image from World Health Organization
This sounds all too familiar with the mood in the US today. Staunch vaccine advocates and Anti-vaccine groups are becoming increasingly angry at one another. Physicians and various others in health care are increasingly divided as well.
Many practices are now refusing to accept Pediatric patients if they aren’t fully vaccinated. Conversely, a few practices even have physicians recommending delayed schedules or opposing them altogether.
There is possibly a potentially big clash coming. How are we to prevent a repeat of the history of Laredo and Plano? Above all, we must understand that while vaccine issues seem large, the implications of loss of liberty and freedom using the guise of the good of the public looms large. What other freedoms do we currently enjoy that might end up on the government chopping block for the “good of all?”
It seems certain considering recent measles and SARS-CoV-2 outbreaks, that if we ostracize anti-vaccine parents and patients, we are going to have government impose the will of those staunchly in favor of vaccines, as they did in Laredo, Texas.
We cannot condone those physicians who give carte blanche anti-vaccine recommendations to patients. It is terrifying to me that state government could begin pulling the licenses of those physicians. And if they do, what other areas such as the care of the aged and dying, or chronically ill or disabled, will be next? The ramifications for government mandated medicine, let alone socialized medicine, are awful.
This sounds all too familiar with the mood in the US today. Staunch vaccine advocates and Anti-vaccine groups are becoming increasingly angry at one another. Physicians and various others in health care are increasingly divided as well.
Many practices are now refusing to accept Pediatric patients if they aren’t fully vaccinated. Conversely, a few practices even have physicians recommending delayed schedules or opposing them altogether.
There is possibly a potentially big clash coming. How are we to prevent a repeat of the history of Laredo and Plano? Above all, we must understand that while vaccine issues seem large, the implications of loss of liberty and freedom using the guise of the good of the public looms large. What other freedoms do we currently enjoy that might end up on the government chopping block for the “good of all?”
It seems certain considering recent measles and SARS-CoV-2 outbreaks, that if we ostracize anti-vaccine parents and patients, we are going to have government impose the will of those staunchly in favor of vaccines, as they did in Laredo, Texas.
We cannot condone those physicians who give carte blanche anti-vaccine recommendations to patients. It is terrifying to me that state government could begin pulling the licenses of those physicians. And if they do, what other areas such as the care of the aged and dying, or chronically ill or disabled, will be next? The ramifications for government mandated medicine, let alone socialized medicine, are awful.
This sounds all too familiar with the mood in the US today. Staunch vaccine advocates and Anti-vaccine groups are becoming increasingly angry at one another. Physicians and various others in health care are increasingly divided as well.
Many practices are now refusing to accept Pediatric patients if they aren’t fully vaccinated. Conversely, a few practices even have physicians recommending delayed schedules or opposing them altogether.
There is possibly a potentially big clash coming. How are we to prevent a repeat of the history of Laredo and Plano? Above all, we must understand that while vaccine issues seem large, the implications of loss of liberty and freedom using the guise of the good of the public looms large. What other freedoms do we currently enjoy that might end up on the government chopping block for the “good of all?”
It seems certain considering recent measles and SARS-CoV-2 outbreaks, that if we ostracize anti-vaccine parents and patients, we are going to have government impose the will of those staunchly in favor of vaccines, as they did in Laredo, Texas.
We cannot condone those physicians who give carte blanche anti-vaccine recommendations to patients. It is terrifying to me that state government could begin pulling the licenses of those physicians. And if they do, what other areas such as the care of the aged and dying, or chronically ill or disabled, will be next? The ramifications for government mandated medicine, let alone socialized medicine, are awful.
- Historical trends in vaccination follow a common pattern.
- Prior to a vaccine, there is a general cry for something to be done.
- Once vaccination begins, there is a quick response and people get vaccinated like crazy.
- As the disease incidence begins to fall as a result, opposition to vaccination begins as general vaccination rates inherently fall.
- Disease caused by the vaccine target then experiences a bloom and vaccination rates pick up
- The cycle can be repeated many times.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
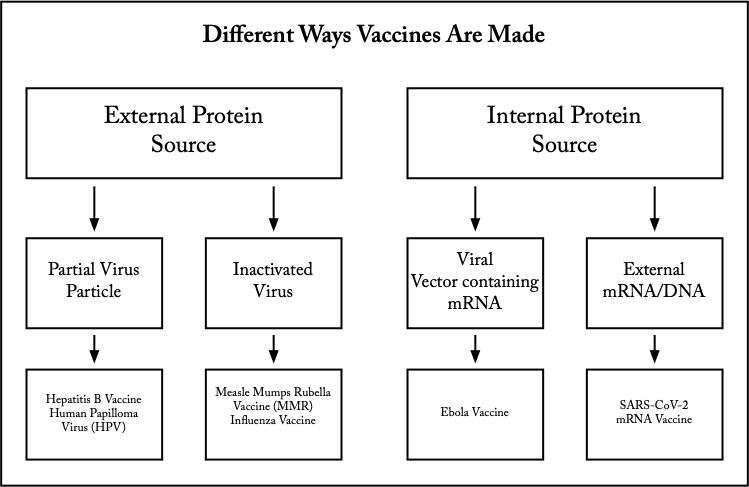
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Edward Jenner’s vaccine for smallpox was actually a whole, live cowpox virus. It is amazing that the vaccine he created worked, because most viruses do not have such similar structural relationship. Only because of that similarity was it effective. His stumbling discovery was the beginning of all future investigations and understanding into contagious infectious disease.
His vaccine was from an external protein source and is known as a whole pathogen vaccine. Unlike smallpox, cowpox didn’t cause serious illness. Most whole pathogen vaccines use inactivated (killed) sources of virus or bacteria. Viruses are inactivated with formaldehyde or heat. They have far fewer proteins than whole cell vaccines like the initial Pertussis (whooping cough) vaccine. Whole cell bacterial vaccines caused far more secondary reactions as a result. Using newer vaccine manufacturing methods have significantly reduced adverse reactions such as fever.
Inactivation, however, reduces the ability of the vaccine to induce host immunity without adding adjuvants like aluminum. Adjuvants increase vaccine effectiveness and reduce the required volume of injected vaccine. Measles-Mumps-Rubella and Influenza vaccines are inactivated virus vaccines.
With the polio vaccine, we discovered the importance of being sure of complete inactivation of whole pathogen vaccines. The failed virus inactivation at one manufacturer became known as the "Cutter incident." Live virus was discovered “hiding” in the vaccine because of the type of filters they were using. Children vaccinated with certain lots of the Cutter vaccine actually contracted polio and some become paralyzed. While no one wanted this, especially Cutter Labs, it highlighted the importance of being sure that whole pathogen vaccines were fully killed by the inactivation process.
Edward Jenner’s vaccine for smallpox was actually a whole, live cowpox virus. It is amazing that the vaccine he created worked, because most viruses do not have such similar structural relationship. Only because of that similarity was it effective. His stumbling discovery was the beginning of all future investigations and understanding into contagious infectious disease.
His vaccine was from an external protein source and is known as a whole pathogen vaccine. Unlike smallpox, cowpox didn’t cause serious illness. Most whole pathogen vaccines use inactivated (killed) sources of virus or bacteria. Viruses are inactivated with formaldehyde or heat. They have far fewer proteins than whole cell vaccines like the initial Pertussis (whooping cough) vaccine. Whole cell bacterial vaccines caused far more secondary reactions as a result. Using newer vaccine manufacturing methods have significantly reduced adverse reactions such as fever.
Inactivation, however, reduces the ability of the vaccine to induce host immunity without adding adjuvants like aluminum. Adjuvants increase vaccine effectiveness and reduce the required volume of injected vaccine. Measles-Mumps-Rubella and Influenza vaccines are inactivated virus vaccines.
With the polio vaccine, we discovered the importance of being sure of complete inactivation of whole pathogen vaccines. The failed virus inactivation at one manufacturer became known as the "Cutter incident." Live virus was discovered “hiding” in the vaccine because of the type of filters they were using. Children vaccinated with certain lots of the Cutter vaccine actually contracted polio and some become paralyzed. While no one wanted this, especially Cutter Labs, it highlighted the importance of being sure that whole pathogen vaccines were fully killed by the inactivation process.
Edward Jenner’s vaccine for smallpox was actually a whole, live cowpox virus. It is amazing that the vaccine he created worked, because most viruses do not have such similar structural relationship. Only because of that similarity was it effective. His stumbling discovery was the beginning of all future investigations and understanding into contagious infectious disease.
His vaccine was from an external protein source and is known as a whole pathogen vaccine. Unlike smallpox, cowpox didn’t cause serious illness. Most whole pathogen vaccines use inactivated (killed) sources of virus or bacteria. Viruses are inactivated with formaldehyde or heat. They have far fewer proteins than whole cell vaccines like the initial Pertussis (whooping cough) vaccine. Whole cell bacterial vaccines caused far more secondary reactions as a result. Using newer vaccine manufacturing methods have significantly reduced adverse reactions such as fever.
Inactivation, however, reduces the ability of the vaccine to induce host immunity without adding adjuvants like aluminum. Adjuvants increase vaccine effectiveness and reduce the required volume of injected vaccine. Measles-Mumps-Rubella and Influenza vaccines are inactivated virus vaccines.
With the polio vaccine, we discovered the importance of being sure of complete inactivation of whole pathogen vaccines. The failed virus inactivation at one manufacturer became known as the "Cutter incident." Live virus was discovered “hiding” in the vaccine because of the type of filters they were using. Children vaccinated with certain lots of the Cutter vaccine actually contracted polio and some become paralyzed. While no one wanted this, especially Cutter Labs, it highlighted the importance of being sure that whole pathogen vaccines were fully killed by the inactivation process.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Inactivated Virus or Bacteria.
The similarity between smallpox and cowpox will perhaps never be repeated. As a result, vaccine solutions for infections like polio and pertussis (whooping cough) moved to using inactivated (also called attenuated) virus and bacteria that could not replicate. The virus or bacteria are essentially killed.
This however was fraught with its own side effects. The DTwP (diphtheria toxin, tetanus toxin, and whole pertussis) vaccine used the entire pertussis bacteria. It was not uncommon to see children with fevers to 103-104°F which came from the myriad of proteins on and in the pertussis cell. The DTaP (with acellular pertussis) vaccine used only some of the proteins, yet the vaccine was equally effective at providing protection.
Partial Virus or Bacteria.
What this meant is that only parts (subunits) of the target virus or bacteria need be used to produce immunity. Later vaccines like the Hib (hemophilus influenza type b bacteria) used this technique and have been famously effective and preventing severe disease with extremely rare side effects. For viral vaccines, it meant that the Cutter incident would never occur since only intact virus within a capsid is infectious.
The only problem with these kinds of vaccines is the length of time to come up with a candidate vaccine which then has to go through Phase I, II, III, and sometimes IV trials. Many trial years leave some victims with serious and permanent residual effects while this testing proceeds. The amazing results with smallpox have not been repeated.
Inactivated Virus or Bacteria.
The similarity between smallpox and cowpox will perhaps never be repeated. As a result, vaccine solutions for infections like polio and pertussis (whooping cough) moved to using inactivated (also called attenuated) virus and bacteria that could not replicate. The virus or bacteria are essentially killed.
This however was fraught with its own side effects. The DTwP (diphtheria toxin, tetanus toxin, and whole pertussis) vaccine used the entire pertussis bacteria. It was not uncommon to see children with fevers to 103-104°F which came from the myriad of proteins on and in the pertussis cell. The DTaP (with acellular pertussis) vaccine used only some of the proteins, yet the vaccine was equally effective at providing protection.
Partial Virus or Bacteria.
What this meant is that only parts (subunits) of the target virus or bacteria need be used to produce immunity. Later vaccines like the Hib (hemophilus influenza type b bacteria) used this technique and have been famously effective and preventing severe disease with extremely rare side effects. For viral vaccines, it meant that the Cutter incident would never occur since only intact virus within a capsid is infectious.
The only problem with these kinds of vaccines is the length of time to come up with a candidate vaccine which then has to go through Phase I, II, III, and sometimes IV trials. Many trial years leave some victims with serious and permanent residual effects while this testing proceeds. The amazing results with smallpox have not been repeated.
Inactivated Virus or Bacteria.
The similarity between smallpox and cowpox will perhaps never be repeated. As a result, vaccine solutions for infections like polio and pertussis (whooping cough) moved to using inactivated (also called attenuated) virus and bacteria that could not replicate. The virus or bacteria are essentially killed.
This however was fraught with its own side effects. The DTwP (diphtheria toxin, tetanus toxin, and whole pertussis) vaccine used the entire pertussis bacteria. It was not uncommon to see children with fevers to 103-104°F which came from the myriad of proteins on and in the pertussis cell. The DTaP (with acellular pertussis) vaccine used only some of the proteins, yet the vaccine was equally effective at providing protection.
Partial Virus or Bacteria.
What this meant is that only parts (subunits) of the target virus or bacteria need be used to produce immunity. Later vaccines like the Hib (hemophilus influenza type b bacteria) used this technique and have been famously effective and preventing severe disease with extremely rare side effects. For viral vaccines, it meant that the Cutter incident would never occur since only intact virus within a capsid is infectious.
The only problem with these kinds of vaccines is the length of time to come up with a candidate vaccine which then has to go through Phase I, II, III, and sometimes IV trials. Many trial years leave some victims with serious and permanent residual effects while this testing proceeds. The amazing results with smallpox have not been repeated.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
External vs Internal Protein Sources for Vaccines.
The partial or subunit protein sources clearly had the advantage over inactivated methods of vaccine development. Still, the time frame for vaccine development was essentially unchanged. Virus for vaccines still required a living host cell to make the multitude of copies required for the mass vaccination of the US population, let alone the world.
The next idea was to use the vaccinated person’s own cellular machinery to produce antigenic protein internally. Injection of the subunit of the target virus or bacteria which produced the immune response was no longer required. Rather, the specific mRNA (or DNA) from the virus or bacteria which coded for the important subunit would be injected.
The advances in genomic analysis in the recent decade have significantly reduced the time to go from subunit protein, to the mRNA that codes for that protein. Cell strains and living tissues, like fertilized chicken eggs, are no longer needed. While the mRNA is very short, it is also extremely temperature sensitive, requiring temperatures of -70° to maintain biologic activity.
Viral Vector Injection of mRNA/DNA.
The cyclic scourge of Ebola in Africa which kills a majority of victims lead to the development of a viral vector vaccine. The mRNA/DNA was inserted into the vector virus DNA. That vector virus would then be injected into the patient where it would infect the host cells. The vector virus itself was one chosen for its harmlessness, so it didn’t cause illness. However, the mRNA/DNA would be carried within the host cell where the ribosomes and tRNA (transfer RNA) would proceed to produce the target viral subunit protein.
Because of this complicated switcheroo, the person getting the vaccine would develop an immunity to the target virus.
External vs Internal Protein Sources for Vaccines.
The partial or subunit protein sources clearly had the advantage over inactivated methods of vaccine development. Still, the time frame for vaccine development was essentially unchanged. Virus for vaccines still required a living host cell to make the multitude of copies required for the mass vaccination of the US population, let alone the world.
The next idea was to use the vaccinated person’s own cellular machinery to produce antigenic protein internally. Injection of the subunit of the target virus or bacteria which produced the immune response was no longer required. Rather, the specific mRNA (or DNA) from the virus or bacteria which coded for the important subunit would be injected.
The advances in genomic analysis in the recent decade have significantly reduced the time to go from subunit protein, to the mRNA that codes for that protein. Cell strains and living tissues, like fertilized chicken eggs, are no longer needed. While the mRNA is very short, it is also extremely temperature sensitive, requiring temperatures of -70° to maintain biologic activity.
Viral Vector Injection of mRNA/DNA.
The cyclic scourge of Ebola in Africa which kills a majority of victims lead to the development of a viral vector vaccine. The mRNA/DNA was inserted into the vector virus DNA. That vector virus would then be injected into the patient where it would infect the host cells. The vector virus itself was one chosen for its harmlessness, so it didn’t cause illness. However, the mRNA/DNA would be carried within the host cell where the ribosomes and tRNA (transfer RNA) would proceed to produce the target viral subunit protein.
Because of this complicated switcheroo, the person getting the vaccine would develop an immunity to the target virus.
External vs Internal Protein Sources for Vaccines.
The partial or subunit protein sources clearly had the advantage over inactivated methods of vaccine development. Still, the time frame for vaccine development was essentially unchanged. Virus for vaccines still required a living host cell to make the multitude of copies required for the mass vaccination of the US population, let alone the world.
The next idea was to use the vaccinated person’s own cellular machinery to produce antigenic protein internally. Injection of the subunit of the target virus or bacteria which produced the immune response was no longer required. Rather, the specific mRNA (or DNA) from the virus or bacteria which coded for the important subunit would be injected.
The advances in genomic analysis in the recent decade have significantly reduced the time to go from subunit protein, to the mRNA that codes for that protein. Cell strains and living tissues, like fertilized chicken eggs, are no longer needed. While the mRNA is very short, it is also extremely temperature sensitive, requiring temperatures of -70° to maintain biologic activity.
Viral Vector Injection of mRNA/DNA.
The cyclic scourge of Ebola in Africa which kills a majority of victims lead to the development of a viral vector vaccine. The mRNA/DNA was inserted into the vector virus DNA. That vector virus would then be injected into the patient where it would infect the host cells. The vector virus itself was one chosen for its harmlessness, so it didn’t cause illness. However, the mRNA/DNA would be carried within the host cell where the ribosomes and tRNA (transfer RNA) would proceed to produce the target viral subunit protein.
Because of this complicated switcheroo, the person getting the vaccine would develop an immunity to the target virus.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
What follows is a general description of mRNA vaccine manufacture. The first step is to identify the section of DNA that codes for the spike protein on the viral capsid. The genome (DNA sequence) for SARS-CoV-2 is published and openly available to everyone. Once the specific spike protein code is identified, then the mRNA sequence from which it is made is created.
The mRNA code is used to create its source DNA code. That DNA is made into a plasmid which is a circular DNA with only the master code for the mRNA which is used to create the spike protein. The plasmid then infects the E. coli bacteria. Plasmids in the world of bacteria are the equivalent of viruses in the animal world. E. coli is an abundant and easily obtainable bacteria. The plasmid DNA then hijacks the E. coli biochemical machinery. That DNA plasmid code begins pouring lots of mRNA which inturn codes for the target spike protein.
This mRNA is collected, purified., and given a protective coating of lipids. Without the lipids, the mRNA would never get into the animal cells.Once inside the cell, the ribosomes, themselves a complex set of protein enzymes, read the vaccine mRNA just like normal mRNA that would come from the cell nucleus. Only the spike protein of the SARS-CoV-2 virus is produced and nothing else. All mRNA has a limited lifespan inside the cells and is quickly degraded.
The spike protein then is what the immune system detects as foreign, just as if the whole virus was present. Antibodies then are created which fend off any real virus attack in the future. A significant number of people seem to already have antibodies that block SARS-CoV-2 from infecting the cells, probably because of exposure to other of the numerous corornaviruses in the wild. Antibodies prevent infection of the cell, but the leftover viral DNA fragments can still produce a positive PCR test.
Mutations occur in all viruses, but this manufacturing process can be quickly adjusted much faster than those for traditional vaccines. The shortest vaccine production in history is the mumps vaccine which took four years to develop. That underscores the value and future of mRNA vaccines.
What follows is a general description of mRNA vaccine manufacture. The first step is to identify the section of DNA that codes for the spike protein on the viral capsid. The genome (DNA sequence) for SARS-CoV-2 is published and openly available to everyone. Once the specific spike protein code is identified, then the mRNA sequence from which it is made is created.
The mRNA code is used to create its source DNA code. That DNA is made into a plasmid which is a circular DNA with only the master code for the mRNA which is used to create the spike protein. The plasmid then infects the E. coli bacteria. Plasmids in the world of bacteria are the equivalent of viruses in the animal world. E. coli is an abundant and easily obtainable bacteria. The plasmid DNA then hijacks the E. coli biochemical machinery. That DNA plasmid code begins pouring lots of mRNA which inturn codes for the target spike protein.
This mRNA is collected, purified., and given a protective coating of lipids. Without the lipids, the mRNA would never get into the animal cells.Once inside the cell, the ribosomes, themselves a complex set of protein enzymes, read the vaccine mRNA just like normal mRNA that would come from the cell nucleus. Only the spike protein of the SARS-CoV-2 virus is produced and nothing else. All mRNA has a limited lifespan inside the cells and is quickly degraded.
The spike protein then is what the immune system detects as foreign, just as if the whole virus was present. Antibodies then are created which fend off any real virus attack in the future. A significant number of people seem to already have antibodies that block SARS-CoV-2 from infecting the cells, probably because of exposure to other of the numerous corornaviruses in the wild. Antibodies prevent infection of the cell, but the leftover viral DNA fragments can still produce a positive PCR test.
Mutations occur in all viruses, but this manufacturing process can be quickly adjusted much faster than those for traditional vaccines. The shortest vaccine production in history is the mumps vaccine which took four years to develop. That underscores the value and future of mRNA vaccines.
What follows is a general description of mRNA vaccine manufacture. The first step is to identify the section of DNA that codes for the spike protein on the viral capsid. The genome (DNA sequence) for SARS-CoV-2 is published and openly available to everyone. Once the specific spike protein code is identified, then the mRNA sequence from which it is made is created.
The mRNA code is used to create its source DNA code. That DNA is made into a plasmid which is a circular DNA with only the master code for the mRNA which is used to create the spike protein. The plasmid then infects the E. coli bacteria. Plasmids in the world of bacteria are the equivalent of viruses in the animal world. E. coli is an abundant and easily obtainable bacteria. The plasmid DNA then hijacks the E. coli biochemical machinery. That DNA plasmid code begins pouring lots of mRNA which inturn codes for the target spike protein.
This mRNA is collected, purified., and given a protective coating of lipids. Without the lipids, the mRNA would never get into the animal cells.Once inside the cell, the ribosomes, themselves a complex set of protein enzymes, read the vaccine mRNA just like normal mRNA that would come from the cell nucleus. Only the spike protein of the SARS-CoV-2 virus is produced and nothing else. All mRNA has a limited lifespan inside the cells and is quickly degraded.
The spike protein then is what the immune system detects as foreign, just as if the whole virus was present. Antibodies then are created which fend off any real virus attack in the future. A significant number of people seem to already have antibodies that block SARS-CoV-2 from infecting the cells, probably because of exposure to other of the numerous corornaviruses in the wild. Antibodies prevent infection of the cell, but the leftover viral DNA fragments can still produce a positive PCR test.
Mutations occur in all viruses, but this manufacturing process can be quickly adjusted much faster than those for traditional vaccines. The shortest vaccine production in history is the mumps vaccine which took four years to develop. That underscores the value and future of mRNA vaccines.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Direct Injection of External mRNA
We now can produce mRNA/DNA strands that code for the important subunit proteins that give our immune system the ability to fight those infections without ever having suffered the diseases themselves. The time from the identification of the best subunit proteins in the virus or bacteria to producing the necessary mRNA/DNA which codes for it is down to a handful of months or less.
Undoubtedly this is the frontier for vaccines and infectious diseases. We are running out of effective antibiotics as fast as we can find new ones. The last, best defense––our own immune system––must become the front line. This will be how we defeat such things as MRSA (multiply resistant staph aureus) and flesh-eating bacteria.
Clinical Trial and Testing
All vaccines require actual clinical trial and testing. Phase I testing involves vaccinating a very small number of healthy people. If all goes well, then Phase II vaccinates a larger group of healthy people. Phase III then vaccinates a very large group of both healthy individuals and those with various chronic diseases.
Initially, these phases are not intended for those who need the protection. The first phases are intended to test the effectiveness of the vaccine and document any side effects. In the later phases, those actually needing the vaccine protection are included in the studies. Phase IV testing may or may not be done. It involves a very, very large number of individuals, and it is often done to show the side effects with the lowest likelihood of occurrence. Pharmaceutical companies often start Phase IV testing at their own discretion after the FDA, following a successful Phase III, has licensed the vaccine.
Direct Injection of External mRNA
We now can produce mRNA/DNA strands that code for the important subunit proteins that give our immune system the ability to fight those infections without ever having suffered the diseases themselves. The time from the identification of the best subunit proteins in the virus or bacteria to producing the necessary mRNA/DNA which codes for it is down to a handful of months or less.
Undoubtedly this is the frontier for vaccines and infectious diseases. We are running out of effective antibiotics as fast as we can find new ones. The last, best defense––our own immune system––must become the front line. This will be how we defeat such things as MRSA (multiply resistant staph aureus) and flesh-eating bacteria.
Clinical Trial and Testing
All vaccines require actual clinical trial and testing. Phase I testing involves vaccinating a very small number of healthy people. If all goes well, then Phase II vaccinates a larger group of healthy people. Phase III then vaccinates a very large group of both healthy individuals and those with various chronic diseases.
Initially, these phases are not intended for those who need the protection. The first phases are intended to test the effectiveness of the vaccine and document any side effects. In the later phases, those actually needing the vaccine protection are included in the studies. Phase IV testing may or may not be done. It involves a very, very large number of individuals, and it is often done to show the side effects with the lowest likelihood of occurrence. Pharmaceutical companies often start Phase IV testing at their own discretion after the FDA, following a successful Phase III, has licensed the vaccine.
Direct Injection of External mRNA
We now can produce mRNA/DNA strands that code for the important subunit proteins that give our immune system the ability to fight those infections without ever having suffered the diseases themselves. The time from the identification of the best subunit proteins in the virus or bacteria to producing the necessary mRNA/DNA which codes for it is down to a handful of months or less.
Undoubtedly this is the frontier for vaccines and infectious diseases. We are running out of effective antibiotics as fast as we can find new ones. The last, best defense––our own immune system––must become the front line. This will be how we defeat such things as MRSA (multiply resistant staph aureus) and flesh-eating bacteria.
Clinical Trial and Testing
All vaccines require actual clinical trial and testing. Phase I testing involves vaccinating a very small number of healthy people. If all goes well, then Phase II vaccinates a larger group of healthy people. Phase III then vaccinates a very large group of both healthy individuals and those with various chronic diseases.
Initially, these phases are not intended for those who need the protection. The first phases are intended to test the effectiveness of the vaccine and document any side effects. In the later phases, those actually needing the vaccine protection are included in the studies. Phase IV testing may or may not be done. It involves a very, very large number of individuals, and it is often done to show the side effects with the lowest likelihood of occurrence. Pharmaceutical companies often start Phase IV testing at their own discretion after the FDA, following a successful Phase III, has licensed the vaccine.
- Smallpox vaccine today is essentially a subunit vaccine, which uses part of a similar virus protein to induce immunity.
- The polio vaccine is made from whole, killed polio virus; it is a whole particle vaccine.
- Newer vaccines are using mRNA technology to make the host cell produce the target antigen only; they cannot cause disease.
- Viral vector vaccines, like that for Ebola, use mRNA attached to a virus which infects the cell and carries the mRNA into the cell.
- Lipid-coated mRNA that is used in the SARS-CoV-2 vaccine is absorbed similarly into the cell as though it were a virus, but it is incapable of causing disease.
- It seems likely that mRNA vaccines will be the wave of the future, since they are highly specific.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
From DNA to Protein.
Used by permission under the Creative Commons Attribution 4.0 CC-BY License. Attribution: yourgenome, (2017). Copyright information available at: https://www.yourgenome.org/copyright.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
From DNA to Protein.
Used by permission under the Creative Commons Attribution 4.0 CC-BY License. Attribution: yourgenome, (2017). Copyright information available at: https://www.yourgenome.org/copyright.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
From DNA to Protein.
Used by permission under the Creative Commons Attribution 4.0 CC-BY License. Attribution: yourgenome, (2017). Copyright information available at: https://www.yourgenome.org/copyright.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
With the first vaccines for SARS-CoV-2 (Coronavirus 2019), you need to have a basic understanding of what mRNA is and what it does. You should watch the explainer video on this slide first.
The mRNA is called messenger RNA because it is a copy of a small gene section of DNA which contains all the master genes. Genes are the master maps, which are the instructions for the linking order of the amino acids that then make all our body’s proteins. Proteins then are the enzymes or structure building blocks which hold us together from the cellular level up to the skin, bones, muscles, ligaments, and organs.
When a virus enters the body, it is first floating free in the fluid between the cells. Viral particles are called capsids. They are extremely small compared to normal body cells and bacteria, and they only have the outer coating and a small strand of mRNA or DNA inside. These small strands of nucleic acids cannot replicate within the capsid like bacterial and normal body cells do. It is only when the capsid touches the outside membrane of the cell or bacteria that it can infect them. Once the virus is inside, it begins to multiply.
The proteins on the outside of the viral capsid attach to proteins on the surface of its target cell, and then the viral capsid fuses with the target cell membrane. The viral mRNA or DNA is then floating free within cell itself.
Viral mRNA then proceeds to the ribosome and makes the viral particle proteins. Either the viral capsids are released at the cell membrane, or the inside of the cell becomes filled with millions of copies of complete viral capsids. When the cell explodes and dies, it releases all the new virus particles.
With the first vaccines for SARS-CoV-2 (Coronavirus 2019), you need to have a basic understanding of what mRNA is and what it does. You should watch the explainer video on this slide first.
The mRNA is called messenger RNA because it is a copy of a small gene section of DNA which contains all the master genes. Genes are the master maps, which are the instructions for the linking order of the amino acids that then make all our body’s proteins. Proteins then are the enzymes or structure building blocks which hold us together from the cellular level up to the skin, bones, muscles, ligaments, and organs.
When a virus enters the body, it is first floating free in the fluid between the cells. Viral particles are called capsids. They are extremely small compared to normal body cells and bacteria, and they only have the outer coating and a small strand of mRNA or DNA inside. These small strands of nucleic acids cannot replicate within the capsid like bacterial and normal body cells do. It is only when the capsid touches the outside membrane of the cell or bacteria that it can infect them. Once the virus is inside, it begins to multiply.
The proteins on the outside of the viral capsid attach to proteins on the surface of its target cell, and then the viral capsid fuses with the target cell membrane. The viral mRNA or DNA is then floating free within cell itself.
Viral mRNA then proceeds to the ribosome and makes the viral particle proteins. Either the viral capsids are released at the cell membrane, or the inside of the cell becomes filled with millions of copies of complete viral capsids. When the cell explodes and dies, it releases all the new virus particles.
With the first vaccines for SARS-CoV-2 (Coronavirus 2019), you need to have a basic understanding of what mRNA is and what it does. You should watch the explainer video on this slide first.
The mRNA is called messenger RNA because it is a copy of a small gene section of DNA which contains all the master genes. Genes are the master maps, which are the instructions for the linking order of the amino acids that then make all our body’s proteins. Proteins then are the enzymes or structure building blocks which hold us together from the cellular level up to the skin, bones, muscles, ligaments, and organs.
When a virus enters the body, it is first floating free in the fluid between the cells. Viral particles are called capsids. They are extremely small compared to normal body cells and bacteria, and they only have the outer coating and a small strand of mRNA or DNA inside. These small strands of nucleic acids cannot replicate within the capsid like bacterial and normal body cells do. It is only when the capsid touches the outside membrane of the cell or bacteria that it can infect them. Once the virus is inside, it begins to multiply.
The proteins on the outside of the viral capsid attach to proteins on the surface of its target cell, and then the viral capsid fuses with the target cell membrane. The viral mRNA or DNA is then floating free within cell itself.
Viral mRNA then proceeds to the ribosome and makes the viral particle proteins. Either the viral capsids are released at the cell membrane, or the inside of the cell becomes filled with millions of copies of complete viral capsids. When the cell explodes and dies, it releases all the new virus particles.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
From DNA to Protein.
Used by permission under the Creative Commons Attribution 4.0 CC-BY License. Attribution: yourgenome, (2017). Copyright information available at: https://www.yourgenome.org/copyright.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
From DNA to Protein.
Used by permission under the Creative Commons Attribution 4.0 CC-BY License. Attribution: yourgenome, (2017). Copyright information available at: https://www.yourgenome.org/copyright.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
From DNA to Protein.
Used by permission under the Creative Commons Attribution 4.0 CC-BY License. Attribution: yourgenome, (2017). Copyright information available at: https://www.yourgenome.org/copyright.
Background: This scanning electron microscope image shows SARS-CoV-2 (yellow)—also known as 2019-nCoV, the virus that causes COVID-19—isolated from a patient in the U.S., emerging from the surface of cells (pink) cultured in the lab. Image captured and colorized at NIAID's Rocky Mountain Laboratories (RML) in Hamilton, Montana. Credit: NIAID
Vaccines that use mRNA can act quickly just like a virus. The mRNA is quickly absorbed into host cells where it quickly starts using the ribosomes and tRNA (transfer RNA) to produce the target protein subunit. This target protein is processed through a series of immune cell interactions which concludes with the B-cell lymphocytes producing antibody against the target subunit protein.
B-cell lymphocytes begin life undifferentiated. That means they have never produced antibodies to any foreign infectious subunit. Once the B-cell becomes “aware” of this foreign subunit protein and produces antibodies to it, it can become less active and produces less antibody over time. This differentiated B-cell will always retain a memory of how to produce that antibody. It will also produce antibodies to only that one foreign protein. It cannot produce antibodies to other foreign infectious proteins.
This is important because sometimes immunity seems to wane over time. The key here though is how we are measuring that immunity. If we are measuring antibody levels against an infection, we cannot be exactly sure that we have lost the memory of how to make those antibodies.
This may be important, for example, in smallpox. Currently vaccine levels are present for about seven years before they wane. What we don’t know then is if smallpox were to break out again, would those like myself who was vaccinated in the 60s be able to mount an immune response and ramp the antibody production back up.
Will mRNA vaccines be able to improve this? Perhaps. One thing is for sure. If we have the genome for an infection, we have much greater leeway to develop a current vaccine to replace older, possibly ineffective, stockpiles for infections like smallpox that we don’t even see in the wild.
Vaccines that use mRNA can act quickly just like a virus. The mRNA is quickly absorbed into host cells where it quickly starts using the ribosomes and tRNA (transfer RNA) to produce the target protein subunit. This target protein is processed through a series of immune cell interactions which concludes with the B-cell lymphocytes producing antibody against the target subunit protein.
B-cell lymphocytes begin life undifferentiated. That means they have never produced antibodies to any foreign infectious subunit. Once the B-cell becomes “aware” of this foreign subunit protein and produces antibodies to it, it can become less active and produces less antibody over time. This differentiated B-cell will always retain a memory of how to produce that antibody. It will also produce antibodies to only that one foreign protein. It cannot produce antibodies to other foreign infectious proteins.
This is important because sometimes immunity seems to wane over time. The key here though is how we are measuring that immunity. If we are measuring antibody levels against an infection, we cannot be exactly sure that we have lost the memory of how to make those antibodies.
This may be important, for example, in smallpox. Currently vaccine levels are present for about seven years before they wane. What we don’t know then is if smallpox were to break out again, would those like myself who was vaccinated in the 60s be able to mount an immune response and ramp the antibody production back up.
Will mRNA vaccines be able to improve this? Perhaps. One thing is for sure. If we have the genome for an infection, we have much greater leeway to develop a current vaccine to replace older, possibly ineffective, stockpiles for infections like smallpox that we don’t even see in the wild.
Vaccines that use mRNA can act quickly just like a virus. The mRNA is quickly absorbed into host cells where it quickly starts using the ribosomes and tRNA (transfer RNA) to produce the target protein subunit. This target protein is processed through a series of immune cell interactions which concludes with the B-cell lymphocytes producing antibody against the target subunit protein.
B-cell lymphocytes begin life undifferentiated. That means they have never produced antibodies to any foreign infectious subunit. Once the B-cell becomes “aware” of this foreign subunit protein and produces antibodies to it, it can become less active and produces less antibody over time. This differentiated B-cell will always retain a memory of how to produce that antibody. It will also produce antibodies to only that one foreign protein. It cannot produce antibodies to other foreign infectious proteins.
This is important because sometimes immunity seems to wane over time. The key here though is how we are measuring that immunity. If we are measuring antibody levels against an infection, we cannot be exactly sure that we have lost the memory of how to make those antibodies.
This may be important, for example, in smallpox. Currently vaccine levels are present for about seven years before they wane. What we don’t know then is if smallpox were to break out again, would those like myself who was vaccinated in the 60s be able to mount an immune response and ramp the antibody production back up.
Will mRNA vaccines be able to improve this? Perhaps. One thing is for sure. If we have the genome for an infection, we have much greater leeway to develop a current vaccine to replace older, possibly ineffective, stockpiles for infections like smallpox that we don’t even see in the wild.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
The SARS-CoV-2 vaccine is NOT the first mRNA vaccine. The Ebola vaccine was the first step toward the mRNA technology. The difference between theses two vaccines is how the target pathogen protein is delivered. The Ebola vaccine is a viral vector vaccine.
The Ebola vaccine uses a virus vector to deliver the target protein itself to the immune cells. The virus vector itself does not injure the cells, while it does deliver the target Ebola protein without the Ebola virus infection.
The Ebola vaccine development started in the 1990s when John “Jack” Rose at Yale used a livestock virus called VSV, or vesicular stomatitis virus. Heinz Feldmann was instrumental in fusing a key Ebola protein onto the VSV at Philipps-University Marburg, Germany, which he later tested in animals before leaving the Canada Nation Microbiology Laboratory in Winnipeg in 2008. Steven Jones, an associate of his whose name is on the Ebola vaccine patent, began development of human-grade vaccine for the initial testing trials.
The FDA approved the Ebola vaccine in 2019. It has proven effective in stopping the spread of Ebola outbreaks. It shows that a target protein from a viral pathogen is effective at stopping the world’s deadliest viral infection, whose mortality rate is at around 70%.
The concern, of course, was that hidden, live and fully infectious VSV virus could be injected into the body. This is not a minor concern. In early polio vaccine development using monkey kidney cells, live and infectious SMV40 virus was discovered in the vaccine. Though it didn’t cause disease in humans, the FDA stopped the further use of non-human cells to cultivate the virus for vaccine production.
The SARS-CoV-2 vaccine is NOT the first mRNA vaccine. The Ebola vaccine was the first step toward the mRNA technology. The difference between theses two vaccines is how the target pathogen protein is delivered. The Ebola vaccine is a viral vector vaccine.
The Ebola vaccine uses a virus vector to deliver the target protein itself to the immune cells. The virus vector itself does not injure the cells, while it does deliver the target Ebola protein without the Ebola virus infection.
The Ebola vaccine development started in the 1990s when John “Jack” Rose at Yale used a livestock virus called VSV, or vesicular stomatitis virus. Heinz Feldmann was instrumental in fusing a key Ebola protein onto the VSV at Philipps-University Marburg, Germany, which he later tested in animals before leaving the Canada Nation Microbiology Laboratory in Winnipeg in 2008. Steven Jones, an associate of his whose name is on the Ebola vaccine patent, began development of human-grade vaccine for the initial testing trials.
The FDA approved the Ebola vaccine in 2019. It has proven effective in stopping the spread of Ebola outbreaks. It shows that a target protein from a viral pathogen is effective at stopping the world’s deadliest viral infection, whose mortality rate is at around 70%.
The concern, of course, was that hidden, live and fully infectious VSV virus could be injected into the body. This is not a minor concern. In early polio vaccine development using monkey kidney cells, live and infectious SMV40 virus was discovered in the vaccine. Though it didn’t cause disease in humans, the FDA stopped the further use of non-human cells to cultivate the virus for vaccine production.
The SARS-CoV-2 vaccine is NOT the first mRNA vaccine. The Ebola vaccine was the first step toward the mRNA technology. The difference between theses two vaccines is how the target pathogen protein is delivered. The Ebola vaccine is a viral vector vaccine.
The Ebola vaccine uses a virus vector to deliver the target protein itself to the immune cells. The virus vector itself does not injure the cells, while it does deliver the target Ebola protein without the Ebola virus infection.
The Ebola vaccine development started in the 1990s when John “Jack” Rose at Yale used a livestock virus called VSV, or vesicular stomatitis virus. Heinz Feldmann was instrumental in fusing a key Ebola protein onto the VSV at Philipps-University Marburg, Germany, which he later tested in animals before leaving the Canada Nation Microbiology Laboratory in Winnipeg in 2008. Steven Jones, an associate of his whose name is on the Ebola vaccine patent, began development of human-grade vaccine for the initial testing trials.
The FDA approved the Ebola vaccine in 2019. It has proven effective in stopping the spread of Ebola outbreaks. It shows that a target protein from a viral pathogen is effective at stopping the world’s deadliest viral infection, whose mortality rate is at around 70%.
The concern, of course, was that hidden, live and fully infectious VSV virus could be injected into the body. This is not a minor concern. In early polio vaccine development using monkey kidney cells, live and infectious SMV40 virus was discovered in the vaccine. Though it didn’t cause disease in humans, the FDA stopped the further use of non-human cells to cultivate the virus for vaccine production.
Why allow a live VSV then for Ebola vaccine? Pure and simple—Ebola mortality is high and has the ability to spread from person to person. The vaccine is only used in the individuals circumferentially close to the index cases.
What the Ebola vaccine taught us is that the target protein approach works and works well. The key to immunity is exposure to the right target protein.
Can we give the target protein itself as the vaccine? Possibly, but there are problems with that approach including local reactions to the injection. If only we could produce the target protein in an evenly distributed way throughout the body, then we could effective a global immunity instead of a local injection reaction.
That is what the mRNA vaccine actually does. Because mRNA is very, very small and is a nucleic acid chain and not an amino acid chain (protein) it seems adverse reactions should be less common. So far that seems to be what we are seeing.
The injection is mRNA which codes for the target protein. When it gets absorbed into cells, it is then used by the existing cellular manufacturing process to produce the target protein. The mRNA degrades and its half-life of is short, so it doesn’t continue on and on indefinitely producing target protein.
The right amount of mRNA in the vaccine causes the normal cells to produce enough target protein for the immune cells to process and develop specific antibodies. The mRNA is contained within a lipid-like coating and is not piggybacked onto a viral vector either. The mRNA does not enter the nucleus of the cell where the DNA is. Even if it did, it would have no effect on the DNA.
mRNA vaccines that have previously been tested in animals include influenza, rabies, and Zika. This technology will speed vaccine production. Time will tell just how effective the immunogenicity is in protecting us.
Why allow a live VSV then for Ebola vaccine? Pure and simple—Ebola mortality is high and has the ability to spread from person to person. The vaccine is only used in the individuals circumferentially close to the index cases.
What the Ebola vaccine taught us is that the target protein approach works and works well. The key to immunity is exposure to the right target protein.
Can we give the target protein itself as the vaccine? Possibly, but there are problems with that approach including local reactions to the injection. If only we could produce the target protein in an evenly distributed way throughout the body, then we could effective a global immunity instead of a local injection reaction.
That is what the mRNA vaccine actually does. Because mRNA is very, very small and is a nucleic acid chain and not an amino acid chain (protein) it seems adverse reactions should be less common. So far that seems to be what we are seeing.
The injection is mRNA which codes for the target protein. When it gets absorbed into cells, it is then used by the existing cellular manufacturing process to produce the target protein. The mRNA degrades and its half-life of is short, so it doesn’t continue on and on indefinitely producing target protein.
The right amount of mRNA in the vaccine causes the normal cells to produce enough target protein for the immune cells to process and develop specific antibodies. The mRNA is contained within a lipid-like coating and is not piggybacked onto a viral vector either. The mRNA does not enter the nucleus of the cell where the DNA is. Even if it did, it would have no effect on the DNA.
mRNA vaccines that have previously been tested in animals include influenza, rabies, and Zika. This technology will speed vaccine production. Time will tell just how effective the immunogenicity is in protecting us.
Why allow a live VSV then for Ebola vaccine? Pure and simple—Ebola mortality is high and has the ability to spread from person to person. The vaccine is only used in the individuals circumferentially close to the index cases.
What the Ebola vaccine taught us is that the target protein approach works and works well. The key to immunity is exposure to the right target protein.
Can we give the target protein itself as the vaccine? Possibly, but there are problems with that approach including local reactions to the injection. If only we could produce the target protein in an evenly distributed way throughout the body, then we could effective a global immunity instead of a local injection reaction.
That is what the mRNA vaccine actually does. Because mRNA is very, very small and is a nucleic acid chain and not an amino acid chain (protein) it seems adverse reactions should be less common. So far that seems to be what we are seeing.
The injection is mRNA which codes for the target protein. When it gets absorbed into cells, it is then used by the existing cellular manufacturing process to produce the target protein. The mRNA degrades and its half-life of is short, so it doesn’t continue on and on indefinitely producing target protein.
The right amount of mRNA in the vaccine causes the normal cells to produce enough target protein for the immune cells to process and develop specific antibodies. The mRNA is contained within a lipid-like coating and is not piggybacked onto a viral vector either. The mRNA does not enter the nucleus of the cell where the DNA is. Even if it did, it would have no effect on the DNA.
mRNA vaccines that have previously been tested in animals include influenza, rabies, and Zika. This technology will speed vaccine production. Time will tell just how effective the immunogenicity is in protecting us.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Katalin Karikó, a Hungarian-born scientist, was a pioneer in pushing mRNA research toward disease prevention in the 1990s. In 1990, the University of Wisconsin proved the idea worked in mice. However, synthetic RNA was very vulnerable to normal body defenses which would destroy it before it could get into the body’s cells. It is only effective if those cells produce the target protein needed to produce immunity against a bacterium or virus.
It was about a decade later that she and Drew Weissman, an immunologist with an MD and Ph.D. from Boston University discovered that by making a slightly hybrid mRNA, these defenses could be skirted. That allowed the mRNA to get into the cells and produce the target protein.
Since then, mRNA technology has been a focus of ground-breaking research. Our confusion then about how quickly these newer vaccines can be produced is what fuels concern about such a short development time.
Traditional vaccine production for viruses takes much longer because the virus has to be grown in quantity, killed, and then used to create the vaccine injection.
The mRNA vaccines don’t rely on living tissues for production. These are very short strings of nucleic acids code for a specific target protein are assembled synthetically. The production process is inherently shorter, therefore, though the vaccine is still effective.
Katalin Karikó, a Hungarian-born scientist, was a pioneer in pushing mRNA research toward disease prevention in the 1990s. In 1990, the University of Wisconsin proved the idea worked in mice. However, synthetic RNA was very vulnerable to normal body defenses which would destroy it before it could get into the body’s cells. It is only effective if those cells produce the target protein needed to produce immunity against a bacterium or virus.
It was about a decade later that she and Drew Weissman, an immunologist with an MD and Ph.D. from Boston University discovered that by making a slightly hybrid mRNA, these defenses could be skirted. That allowed the mRNA to get into the cells and produce the target protein.
Since then, mRNA technology has been a focus of ground-breaking research. Our confusion then about how quickly these newer vaccines can be produced is what fuels concern about such a short development time.
Traditional vaccine production for viruses takes much longer because the virus has to be grown in quantity, killed, and then used to create the vaccine injection.
The mRNA vaccines don’t rely on living tissues for production. These are very short strings of nucleic acids code for a specific target protein are assembled synthetically. The production process is inherently shorter, therefore, though the vaccine is still effective.
Katalin Karikó, a Hungarian-born scientist, was a pioneer in pushing mRNA research toward disease prevention in the 1990s. In 1990, the University of Wisconsin proved the idea worked in mice. However, synthetic RNA was very vulnerable to normal body defenses which would destroy it before it could get into the body’s cells. It is only effective if those cells produce the target protein needed to produce immunity against a bacterium or virus.
It was about a decade later that she and Drew Weissman, an immunologist with an MD and Ph.D. from Boston University discovered that by making a slightly hybrid mRNA, these defenses could be skirted. That allowed the mRNA to get into the cells and produce the target protein.
Since then, mRNA technology has been a focus of ground-breaking research. Our confusion then about how quickly these newer vaccines can be produced is what fuels concern about such a short development time.
Traditional vaccine production for viruses takes much longer because the virus has to be grown in quantity, killed, and then used to create the vaccine injection.
The mRNA vaccines don’t rely on living tissues for production. These are very short strings of nucleic acids code for a specific target protein are assembled synthetically. The production process is inherently shorter, therefore, though the vaccine is still effective.
Maybe so, but only time will tell. There would likely be some immunity. We should be able to quickly figure out the new mRNA code needed to create new target virus proteins, from which we can update the vaccine. Unlike drug-resistant bacteria and viruses, which can take years to figure out newer effect drugs, we have an advantage.
Maybe so, but only time will tell. There would likely be some immunity. We should be able to quickly figure out the new mRNA code needed to create new target virus proteins, from which we can update the vaccine. Unlike drug-resistant bacteria and viruses, which can take years to figure out newer effect drugs, we have an advantage.
Maybe so, but only time will tell. There would likely be some immunity. We should be able to quickly figure out the new mRNA code needed to create new target virus proteins, from which we can update the vaccine. Unlike drug-resistant bacteria and viruses, which can take years to figure out newer effect drugs, we have an advantage.
There is no evidence that mRNA vaccines cause infertility in women. More studies will come, for sure. However, my gut feeling is that they are safe. Because the vaccine is currently under an emergent use authorization, it is appropriate to be cautious. It is not yet approved in children. They seem to be at the least risk for any symptoms if they are getting infected much at all.
There is no evidence that mRNA vaccines cause infertility in women. More studies will come, for sure. However, my gut feeling is that they are safe. Because the vaccine is currently under an emergent use authorization, it is appropriate to be cautious. It is not yet approved in children. They seem to be at the least risk for any symptoms if they are getting infected much at all.
There is no evidence that mRNA vaccines cause infertility in women. More studies will come, for sure. However, my gut feeling is that they are safe. Because the vaccine is currently under an emergent use authorization, it is appropriate to be cautious. It is not yet approved in children. They seem to be at the least risk for any symptoms if they are getting infected much at all.
I’m not familiar with any serious risks beyond those common for any type of injection, vaccine or otherwise. So far, the observed medical adverse reactions seem to be very low. Most of the talk of risks and side effects is unfounded.
Local reactions are a risk with all injections. Fainting is something very commonly observed after any injection. This is a vasovagal response usually, which is not related to the content of the injection.
I come from the perspective of having seen 4-6 kids a month with temps of 104 or more who were vaccinated with DTwP (whole-cell pertussis vaccine). Today, I might see 4-6 kids over 2 or 3 years, or more, with those elevated vaccine-induced temps.
So far, the phased trials have not shown interactions with other medications. That doesn’t mean we might not see some when we start getting into the 100 of millions of administered doses. However, that would be the case with all medications and injectables.
I’m not familiar with any serious risks beyond those common for any type of injection, vaccine or otherwise. So far, the observed medical adverse reactions seem to be very low. Most of the talk of risks and side effects is unfounded.
Local reactions are a risk with all injections. Fainting is something very commonly observed after any injection. This is a vasovagal response usually, which is not related to the content of the injection.
I come from the perspective of having seen 4-6 kids a month with temps of 104 or more who were vaccinated with DTwP (whole-cell pertussis vaccine). Today, I might see 4-6 kids over 2 or 3 years, or more, with those elevated vaccine-induced temps.
So far, the phased trials have not shown interactions with other medications. That doesn’t mean we might not see some when we start getting into the 100 of millions of administered doses. However, that would be the case with all medications and injectables.
I’m not familiar with any serious risks beyond those common for any type of injection, vaccine or otherwise. So far, the observed medical adverse reactions seem to be very low. Most of the talk of risks and side effects is unfounded.
Local reactions are a risk with all injections. Fainting is something very commonly observed after any injection. This is a vasovagal response usually, which is not related to the content of the injection.
I come from the perspective of having seen 4-6 kids a month with temps of 104 or more who were vaccinated with DTwP (whole-cell pertussis vaccine). Today, I might see 4-6 kids over 2 or 3 years, or more, with those elevated vaccine-induced temps.
So far, the phased trials have not shown interactions with other medications. That doesn’t mean we might not see some when we start getting into the 100 of millions of administered doses. However, that would be the case with all medications and injectables.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
The FDA authorized the mRNA vaccine under the emergent use conditions based on phase I, phase II, and phase III trials. When we have administered millions upon millions of doses beyond the phased trials, the FDA could revoke the use of the vaccine should reactions occur that were not observed in the trials with a relatively smaller number of vaccinees.
I remember the rotavirus vaccine which was intended to prevent rotaviral diarrhea and dehydration common in less developed countries. When it first came out, everyone was excited it seemed, but I was hesitant, especially since it wasn’t a required vaccination for school.
It turned out that it was so immunogenic, that it caused lymph nodes along the intestine to enlarge significantly. These lymph nodes caused the bowel to intussuscept into itself like a sock. This intussusception caused bowel obstruction, a serious condition . Significant numbers of children required surgical decompression when barium enemas failed to relieve the blockage. A few kids even died from the intussusception, though not directly from the vaccine itself.
The FDA pulled the vaccine within a year. It was reworked, and new clinical trials and ultimately proved that the intussusception problem was resolved. While that experience shook up many physicians, the vaccine today has proven safe and effective.
Just because a vaccine or medication is approved and in use for many years, the FDA is always watching. Several drugs that worked very, very well have been pulled after many, many years of use. This doesn’t mean the approval was wrong at the time. It means that greater knowledge later demonstrated unknown side effects. Such will always be the case with all medications.
The FDA authorized the mRNA vaccine under the emergent use conditions based on phase I, phase II, and phase III trials. When we have administered millions upon millions of doses beyond the phased trials, the FDA could revoke the use of the vaccine should reactions occur that were not observed in the trials with a relatively smaller number of vaccinees.
I remember the rotavirus vaccine which was intended to prevent rotaviral diarrhea and dehydration common in less developed countries. When it first came out, everyone was excited it seemed, but I was hesitant, especially since it wasn’t a required vaccination for school.
It turned out that it was so immunogenic, that it caused lymph nodes along the intestine to enlarge significantly. These lymph nodes caused the bowel to intussuscept into itself like a sock. This intussusception caused bowel obstruction, a serious condition . Significant numbers of children required surgical decompression when barium enemas failed to relieve the blockage. A few kids even died from the intussusception, though not directly from the vaccine itself.
The FDA pulled the vaccine within a year. It was reworked, and new clinical trials and ultimately proved that the intussusception problem was resolved. While that experience shook up many physicians, the vaccine today has proven safe and effective.
Just because a vaccine or medication is approved and in use for many years, the FDA is always watching. Several drugs that worked very, very well have been pulled after many, many years of use. This doesn’t mean the approval was wrong at the time. It means that greater knowledge later demonstrated unknown side effects. Such will always be the case with all medications.
The FDA authorized the mRNA vaccine under the emergent use conditions based on phase I, phase II, and phase III trials. When we have administered millions upon millions of doses beyond the phased trials, the FDA could revoke the use of the vaccine should reactions occur that were not observed in the trials with a relatively smaller number of vaccinees.
I remember the rotavirus vaccine which was intended to prevent rotaviral diarrhea and dehydration common in less developed countries. When it first came out, everyone was excited it seemed, but I was hesitant, especially since it wasn’t a required vaccination for school.
It turned out that it was so immunogenic, that it caused lymph nodes along the intestine to enlarge significantly. These lymph nodes caused the bowel to intussuscept into itself like a sock. This intussusception caused bowel obstruction, a serious condition . Significant numbers of children required surgical decompression when barium enemas failed to relieve the blockage. A few kids even died from the intussusception, though not directly from the vaccine itself.
The FDA pulled the vaccine within a year. It was reworked, and new clinical trials and ultimately proved that the intussusception problem was resolved. While that experience shook up many physicians, the vaccine today has proven safe and effective.
Just because a vaccine or medication is approved and in use for many years, the FDA is always watching. Several drugs that worked very, very well have been pulled after many, many years of use. This doesn’t mean the approval was wrong at the time. It means that greater knowledge later demonstrated unknown side effects. Such will always be the case with all medications.
This is not a reason to berate the mRNA vaccine. We know nothing about any vaccine’s immunogenicity until we start giving it publicly. How we determine the level of immunity can be an issue too. We know that there are a high number of false-positive PCR tests for SARS-CoV-2. Individuals who tested positive, who weren’t ill with symptoms, probably were never infected with the virus at the cellular level. If you have blocking antibodies that prevent cellular infection, you can still have a positive PCR. You would not be contagious and should not be considered clinically infected.
Are antibody levels proof that a person’s immunity has waned? Absolutely not! We maintain immunologic memory of infection even when antibody levels may be low. Challenges by bacteria or virus can result in sudden and brisk increase in the antibody levels. Such was the case with the H1N1 Spanish flu in the late 2000s. It affected the younger adolescents, but because the virus was prevalent in my 1960s childhood, I was protected.
Every vaccine and target virus are different how long immunity lasts. Smallpox vaccine may only be good for about 7 years, but we are not sure since there is no smallpox in the wild. Yellow fever vaccine is good for thirty years!
Why the difference? I don’t think anyone is sure, but were smallpox back in the wild, we wouldn’t refuse to get the current smallpox vaccine, were it available to the general public, because we thought it would only last 7 years.
Granted, smallpox is much more serious than SARS-CoV-2, but I think you get my point.
This is not a reason to berate the mRNA vaccine. We know nothing about any vaccine’s immunogenicity until we start giving it publicly. How we determine the level of immunity can be an issue too. We know that there are a high number of false-positive PCR tests for SARS-CoV-2. Individuals who tested positive, who weren’t ill with symptoms, probably were never infected with the virus at the cellular level. If you have blocking antibodies that prevent cellular infection, you can still have a positive PCR. You would not be contagious and should not be considered clinically infected.
Are antibody levels proof that a person’s immunity has waned? Absolutely not! We maintain immunologic memory of infection even when antibody levels may be low. Challenges by bacteria or virus can result in sudden and brisk increase in the antibody levels. Such was the case with the H1N1 Spanish flu in the late 2000s. It affected the younger adolescents, but because the virus was prevalent in my 1960s childhood, I was protected.
Every vaccine and target virus are different how long immunity lasts. Smallpox vaccine may only be good for about 7 years, but we are not sure since there is no smallpox in the wild. Yellow fever vaccine is good for thirty years!
Why the difference? I don’t think anyone is sure, but were smallpox back in the wild, we wouldn’t refuse to get the current smallpox vaccine, were it available to the general public, because we thought it would only last 7 years.
Granted, smallpox is much more serious than SARS-CoV-2, but I think you get my point.
This is not a reason to berate the mRNA vaccine. We know nothing about any vaccine’s immunogenicity until we start giving it publicly. How we determine the level of immunity can be an issue too. We know that there are a high number of false-positive PCR tests for SARS-CoV-2. Individuals who tested positive, who weren’t ill with symptoms, probably were never infected with the virus at the cellular level. If you have blocking antibodies that prevent cellular infection, you can still have a positive PCR. You would not be contagious and should not be considered clinically infected.
Are antibody levels proof that a person’s immunity has waned? Absolutely not! We maintain immunologic memory of infection even when antibody levels may be low. Challenges by bacteria or virus can result in sudden and brisk increase in the antibody levels. Such was the case with the H1N1 Spanish flu in the late 2000s. It affected the younger adolescents, but because the virus was prevalent in my 1960s childhood, I was protected.
Every vaccine and target virus are different how long immunity lasts. Smallpox vaccine may only be good for about 7 years, but we are not sure since there is no smallpox in the wild. Yellow fever vaccine is good for thirty years!
Why the difference? I don’t think anyone is sure, but were smallpox back in the wild, we wouldn’t refuse to get the current smallpox vaccine, were it available to the general public, because we thought it would only last 7 years.
Granted, smallpox is much more serious than SARS-CoV-2, but I think you get my point.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
Copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
All slides copyright © 2020 and beyond by Ron Smith, MD. All rights reserved.
There is a big difference between DNA and RNA. In particular, the chain of nucleotides in DNA consists of adenosine, thymine, cytosine, and guanine. Uracil replaces thymine in mRNA.
The whole of the mRNA, a string strand of specific nucleotides, is a code for only one protein. DNA has two strands running in opposite directions with cross links between each strand. It is the master map for all the proteins your body can make. It is unwound, and then an mRNA for a single protein is created from its map.
Additionally, the nucleotides in DNA that are cross-linked must match up correctly. Adenosine will only cross-link with thymine. Cytosine can only connect to guanine. There are no cross links in mRNA. Look at this instructional video which explains this visually.
It is clear, then, that mRNA cannot change, replace, or act as DNA. That one difference in nucleotides prevents mRNA from ever functioning like DNA. Breakdowns in DNA can and do occur, such as with exposure to ionizing radiation. The double stranded nature is a clever structure that ensure it always has a backup copy to repair it, so long as one strand remains fully intact.
Now you are ready to take the quiz.
There is a big difference between DNA and RNA. In particular, the chain of nucleotides in DNA consists of adenosine, thymine, cytosine, and guanine. Uracil replaces thymine in mRNA.
The whole of the mRNA, a string strand of specific nucleotides, is a code for only one protein. DNA has two strands running in opposite directions with cross links between each strand. It is the master map for all the proteins your body can make. It is unwound, and then an mRNA for a single protein is created from its map.Additionally, the nucleotides in DNA that are cross-linked must match up correctly. Adenosine will only cross-link with thymine. Cytosine can only connect to guanine. There are no cross links in mRNA. Look at this instructional video which explains this visually.
It is clear, then, that mRNA cannot change, replace, or act as DNA. That one difference in nucleotides prevents mRNA from ever functioning like DNA. Breakdowns in DNA can and do occur, such as with exposure to ionizing radiation. The double stranded nature is a clever structure that ensure it always has a backup copy to repair it, so long as one strand remains fully intact.
Now you are ready to take the quiz.
There is a big difference between DNA and RNA. In particular, the chain of nucleotides in DNA consists of adenosine, thymine, cytosine, and guanine. Uracil replaces thymine in mRNA.
The whole of the mRNA, a string strand of specific nucleotides, is a code for only one protein. DNA has two strands running in opposite directions with cross links between each strand. It is the master map for all the proteins your body can make. It is unwound, and then an mRNA for a single protein is created from its map.
Additionally, the nucleotides in DNA that are cross-linked must match up correctly. Adenosine will only cross-link with thymine. Cytosine can only connect to guanine. There are no cross links in mRNA. Look at this instructional video which explains this visually.
It is clear, then, that mRNA cannot change, replace, or act as DNA. That one difference in nucleotides prevents mRNA from ever functioning like DNA. Breakdowns in DNA can and do occur, such as with exposure to ionizing radiation. The double stranded nature is a clever structure that ensure it always has a backup copy to repair it, so long as one strand remains fully intact.
Now you are ready to take the quiz.
Used by permission. http://www.AmoebaSisters.com
